Протезно кероване розміщення імплантату: індивідуалізовані техніки регенерації кістки з кастомізованими титановими сітками Yxoss CBR
Машинний переклад
Оригінальна стаття написана мовою IT (посилання для прочитання) .
Розміщення зубного імплантату є ефективним лікуванням для заміни втрачених зубів, з високими показниками виживання імплантів у довгостроковій перспективі.
Основним фактором успіху імплантології є наявність адекватної кісткової структури. Щоб зубні імпланти були успішними, кістка повинна бути достатньою як кількісно (щодо висоти та/або ширини), так і якісно (широка васкуляризація).
Відсутність адекватного обсягу кістки є поширеним стримуючим фактором для розміщення зубних імплантів і також причиною невдачі імплантації, як на етапі загоєння/остеоінтеграції, так і на етапі реставрації.
Отже, адекватний обсяг кістки є важливим передумовою для прогнозування довгострокового успіху в імплантології та для функціонально і естетично правильної реабілітації. Залишковий обсяг кістки часто є недостатнім для дозволу вставки зубних імплантів відповідно до критеріїв протезної імплантології, як зазначено в останніх рекомендаціях. Тому відновлення адекватної кількості кістки та адекватного контурів альвеолярного гребеня повинні бути враховані в будь-якому плані лікування, щоб дозволити розміщення імпланту, керуючись протезуванням.
Бар'єрні мембрани використовуються в стоматологічній імплантології з кінця 1980-х років у процедурі керованої регенерації кістки (GBR). Такий бар'єр має на меті запобігти внутрішньому росту клітин сполучної тканини, що не є остеогенними, у кістковому дефекті та створити простір, в якому може організуватися кров'яний згусток з подальшим утворенням нової кістки. Ідеальні характеристики мембрани включають: біосумісність, легкість маніпуляції, інтеграцію з навколишніми тканинами, підтримання простору та стабілізацію рани.
Управління м'якими тканинами є одним з ключових моментів GBR. Закриття рани первинним швом без напруги є обов'язковим при виконанні будь-якої процедури збільшення кістки. В іншому випадку відбудеться раннє розкриття рани.
Керована регенерація кістки може бути виконана двома способами:
- Двохетапна процедура: спочатку виконується GBR, а через 4-9 місяців імплантат може бути вставлений у правильну 3D позицію в кістці, що заживає;
- Одноетапна процедура: імплантат вставляється одночасно з регенерацією кістки; ця процедура є здійсненною, коли імплантат може бути вставлений у правильну 3D позицію з достатньою первинною стабільністю та з закриттям рани первинним швом без напруги.
Використання титанових сіток у керованій регенерації кістки є поширеною процедурою для збільшення горизонтального та вертикального гребеня. Клінічний та гістологічний аналіз виявив збільшення гребеня та формування нової кістки після застосування титанової сітки разом з депротейнізованим (DBBM) коров’ячим кістковим мінералом та аутологічною кісткою. Можна досягти більшого вертикального приросту гребеня, використовуючи титанові сітки. Основним недоліком традиційних титанових сіток є ручне 3-D різання під час операції, що займає багато часу для досягнення бажаної остаточної форми.
Сьогодні технологію CAD/CAM можна використовувати для подолання цих недоліків. Використовуючи комп'ютерну томографію (КТ) окремого пацієнта або конусно-променеву комп'ютерну томографію (CBCT), обсяг збільшення, необхідний для дефектів, можна оцінити на передопераційному етапі, що дозволяє створити дефектоспецифічну сітку. Індивідуально виготовлені титанові сітки Yxoss CBR виготовляються з використанням даних DICOM пацієнта, щоб уникнути підгонки традиційних титанових сіток під час операції. Застосування індивідуально виготовленої сітки скорочує час операції і може зменшити загальні витрати на лікування. Найпоширенішою ускладненням титанових сіток є деісценція клаптя. Sagheb та ін. опублікували дослідження про використання індивідуально виготовлених титанових сіток Yxoss CBR для збільшення альвеолярного гребеня і продемонстрували, що немає жодного негативного впливу можливих деісценцій на результати лікування.
Seiler та ін. повідомили про лікування 115 дефектів альвеолярного гребеня, реконструйованих з використанням сіток Yxoss CBR у поєднанні з частинками аутологічної кістки та DBBM, з або без покриття мембраною з натурального колагену. Дослідження показало загоєння без ускладнень у 82 дефектах. Інфекція хірургічної області була задокументована в 11 випадках, з яких 10 були вирішені за допомогою медикаментів. Деісценція була зафіксована в 26 дефектах (рівень експозиції 22,6%). Передчасне видалення відкритих сіток не було необхідним. Усі випадки продемонстрували достатню регенерацію кістки для встановлення імплантату з попереднім 3-D плануванням. Об'єм трансплантату в дефектах з деісценцією не відрізнявся від об'єму в ділянках без деісценції. Статистичний аналіз не виявив жодної кореляції між деісценцією та демографічними або хірургічними параметрами, але спостерігалася тенденція до більшої поширеності деісценції з ростом мезіо-дистальної ширини дефекта. Вони, отже, зробили висновок, що комбінація сітки з титану на замовлення Yxoss CBR з керованою регенерацією кістки є надійною технікою трансплантації з низькою чутливістю до деісценції.
Нещодавно дослідження Чіапаско та ін. підтвердило результати щодо рівня експозиції. З загальної кількості 53 ділянок, оброблених титановими решітками на замовлення Yxoss CBR та сумішшю аутологічної кістки і DBBM, 11 показали експозицію решіток (рівень експозиції 20,75%): у 8 з них інтеграція трансплантату відбулася без проблем, тоді як у 3 спостерігалася часткова втрата кістки. На ділянках, які зазнали часткової втрати кістки, все ж було можливим виконати заплановані протезування. Робота також продемонструвала високий приріст кістки (середнє вертикальне та горизонтальне збільшення кістки становило відповідно 4,78±1,88 мм та 6,35±2,10 мм) та рівень виживання імплантатів 100%22. Делавія та ін. провели гістологічний аналіз регенерованої кістки з решітками Yxoss CBR у поєднанні з сумішшю аутологічної кістки та DBBM через 9 місяців після загоєння. У всіх ділянках новоутворена тканина виявилася високо мінералізованою, добре організованою і складалася з 35,88% нової ламелярної кістки, 16,42% кістки з переплетеними волокнами, 10,88% остеоїдної матриці, 14,10% залишків трансплантату та 22,72% кісткових порожнин. Судини становили 4% тканини. Ці дані продемонстрували, що регенерація з решітками Yxoss CBR у поєднанні з аутологічною кісткою та DBBM дозволяє досягти адекватної васкуляризації та життєздатності регенерованої кістки.
Крім того, навіть у випадку GBR для лікування великих дефектів з використанням сітки Yxoss CBR у поєднанні з сумішшю аутологічної кістки та DBBM, у співвідношенні на користь останньої, якість новоутвореної кістки є оптимальною.
У клінічному випадку, описаному Гароччо, опублікованому в Implants, результати гістологічного дослідження, проведеного через дев'ять місяців після втручання з використанням індивідуальних титанових сіток Yxoss CBR, показали, що кістка має нормальну морфологію, що характеризується новоутвореними кістковими трабекулами, які обмежують великі кісткові простори, багаті судинами. Остеокластичні клітини не були виявлені, що свідчить про те, що ремоделювання є мінімальним, а кістка знаходиться на просунутій стадії організації та зрілості.
Клінічний випадок
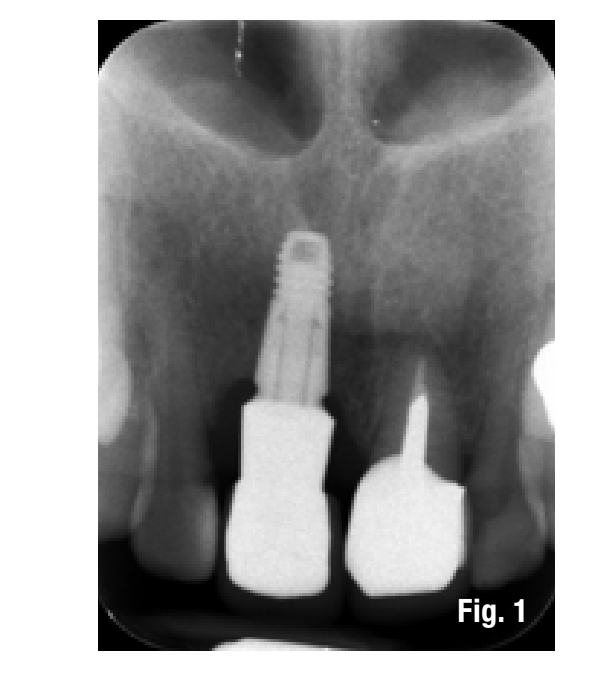
Пацієнтка звертається до нас зі скаргами на естетичний дискомфорт і часті абсцесні епізоди. У зоні 1.1 ми виявляємо наявність імплантованого реставраційного елемента та постійне рішення на рівні вестибулярної маргінальної ясен. При рентгенографічному обстеженні виявляється значна втрата кістки, пов'язана також з неправильним розташуванням імплантату. Надмірна глибина введення імплантату та неправильне управління трансмукозним шляхом призвели до естетичної та функціональної шкоди (Рис. 1-3).


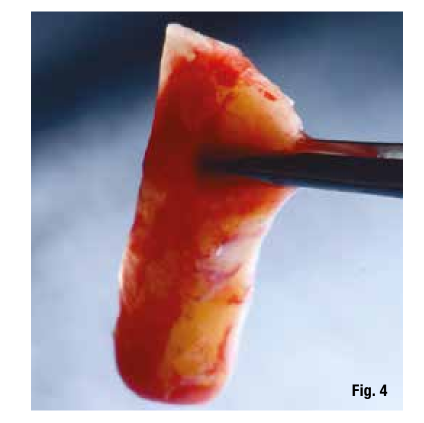
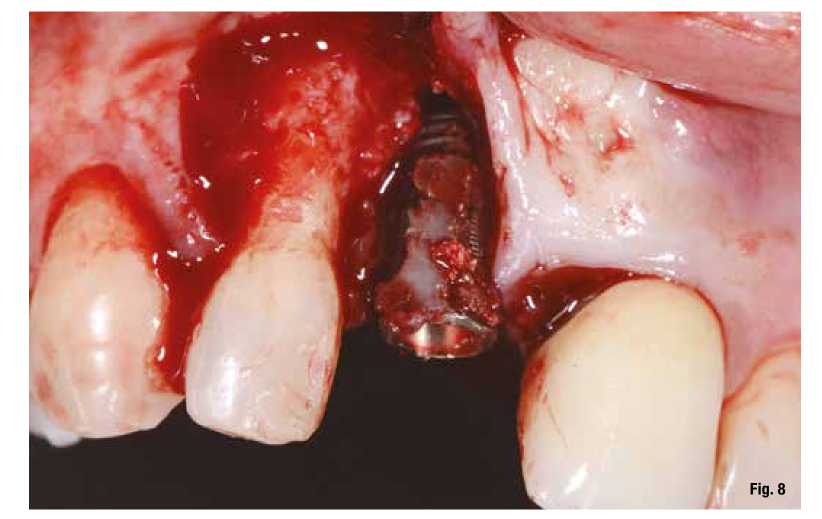
Запланований план лікування передбачає видалення імплантату та управління залишковим дефектом за допомогою техніки GBR. Незалежно від обраної техніки, для правильного управління регенеративними процедурами нам потрібна якість і кількість м'яких тканин, достатня для підтримки покриття дефекту. При аналізі ділянки, що підлягає лікуванню, ми виявляємо повну відсутність прикріпленої ясеневої тканини, і тому плануємо збільшення тканини за допомогою використання вільного ясеневого трансплантату (Рис. 4, 5). Для дозрівання м'яких тканин ми чекали три місяці перед тим, як перейти до видалення імплантату (Рис. 6). У таких випадках видалення імплантату ускладнене і супроводжується подальшою втратою кістки. Після видалення імплантату ми можемо краще оцінити неправильне лікування імплантно-протезного комплексу (Рис. 7-9). Ми чекаємо приблизно три місяці, і в цей час починаємо проектувати регенеративну техніку. Ми робимо це, аналізуючи CBCT та програмне забезпечення для направленої хірургії, яке дозволяє нам зрозуміти обсяг необхідної регенерації кістки. Протягом тривалого часу, щоб спростити та зробити передбачуваною регенеративну техніку, ми використовуємо титанові решітки, які виготовляються на основі конусно-променевих зображень, воскових моделей та вказівок, які ми надаємо виробнику.




Проектування відновлення кістки було виконано таким чином, що воно керується протезами, розміщуючи віртуальний імплант і оцінюючи обсяг необхідної регенерації.
Отримавши всю необхідну інформацію про кісткові дані (конусно-променева томографія) та протезування (STL воскової моделі, тканин і початкової ситуації), ми надсилаємо все компанії (ReOss, Фільдерштадт), яка після проектування надсилає нам дизайн решітки Yxoss CBR, яку можна переглядати в тривимірному форматі та за необхідності змінювати на розсуд професіонала. Після внесення можливих змін виконується фінальна валідація проекту для виготовлення решітки (Рис. 10). Завдяки Customized Bone Regeneration (CBR) мета цифрової регенерації, керованої протезами, досягається.
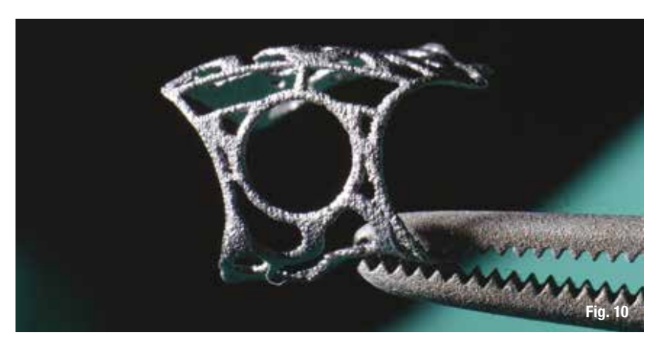
Сітки виготовляються за допомогою тривимірного друку, і їхнє прилягання до дефекту завжди дуже точне, це дозволяє зосередити увагу на інших етапах хірургії.
Управління втручанням стає дуже простим, наша увага повинна бути спрямована на правильний малюнок клаптя, оскільки, маючи в розпорядженні сітку, специфічну для дефекту, ми не повинні витрачати час на вирізання мембран або класичних титанових сіток. Первинний розріз клаптя відрізняється від того, який ми зазвичай робимо для процедур GBR з мембранами. Перший розріз робиться на гребені або, в деяких випадках, навіть більш вестибулярно до дефекту. Таким чином, ми залишаємо більше піднебінного тканини для покриття сітки, а вестибулярний клапоть пасивовано через маневри періостальних і м'язових вивільнень.
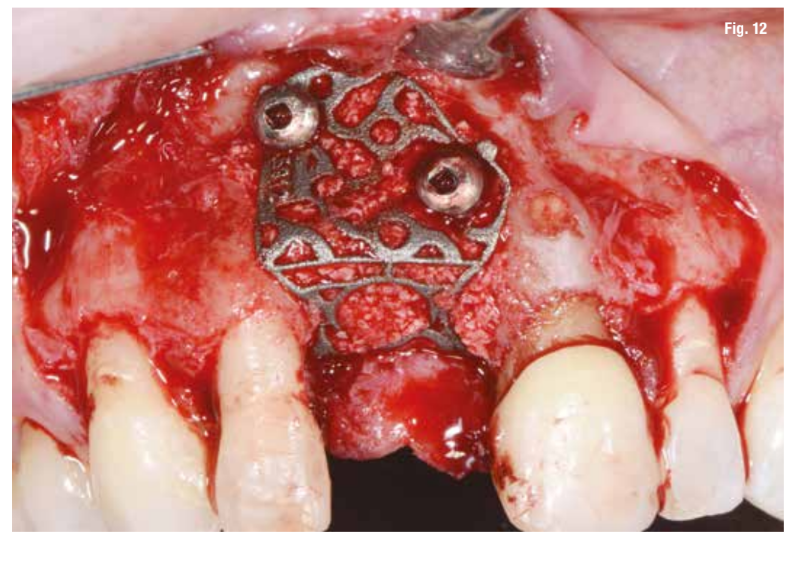
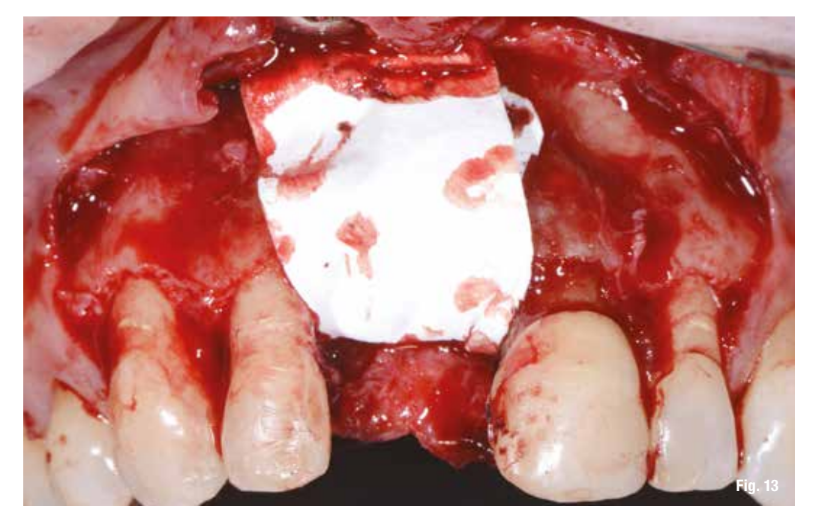
Після виконання дебридменту дефекту (Рис. 11), спочатку перевіряємо прилягання сітки, а потім заповнюємо її сумішшю аутологічної кістки, зібраної за допомогою Safe Scraper, та 50% депротенізованого коров'ячого кісткового мінералу (Geistlich Bio-Oss, Geistlich Pharma AG). Сітка потім фіксується міні-гвинтами (Рис. 12) і покривається розсмоктувальною колагеновою мембраною (Geistlich Bio-Gide, Geistlich Pharma AG), щоб покращити загоєння тканин і запобігти міграції м'якої тканини всередину трансплантату (Рис. 13).

Лоскут, після того як його звільнили від періосту та м'язових шарів, повторно розміщується без напруги. Шви виконуються з горизонтальними матрацними швами, поєднаними з окремими швами на поверхні лоскута, що забезпечує закриття рани з першого разу (Рис. 14).

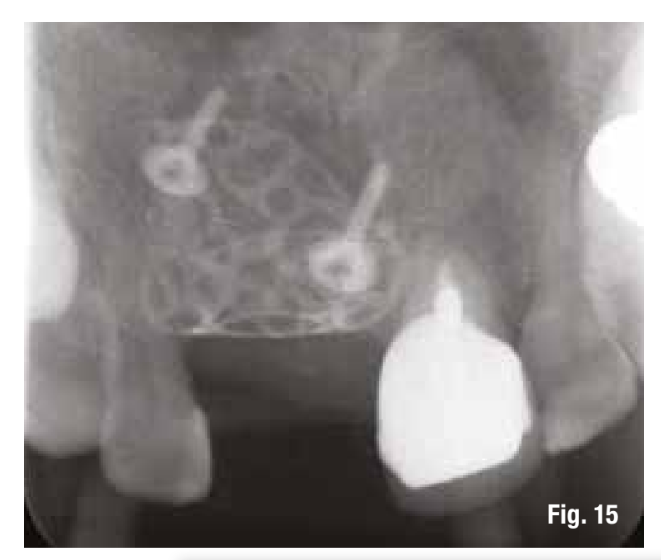
Фундаментальним є контроль післяопераційного стану (Рис. 15). Шви знімаються через 15 днів, а контроль через місяць показує хороше загоєння тканин.
Перед тим як перейти до імплантації, ми змінюємо колір трансплантата за допомогою простої хірургічної техніки (Рис. 16).

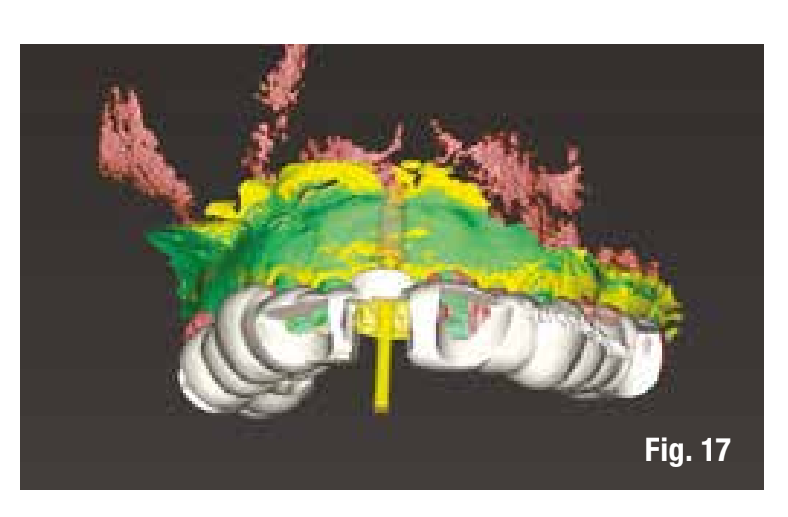
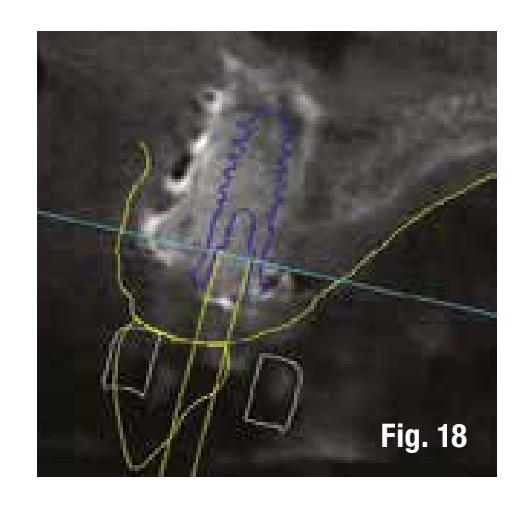
Щоб зменшити кількість втручань, ми плануємо імплантацію, керуючись протезуванням, за допомогою комп'ютерної хірургії, яка буде виконана після видалення решітки. Зображення в програмному забезпеченні дозволяють нам вставити імплантат в регенеровану кістку у спосіб, керуючись протезуванням (Рис. 17, 18).
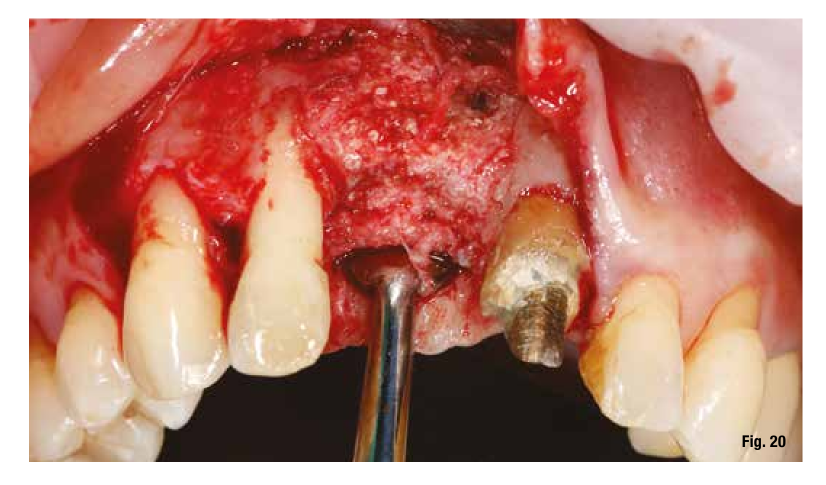
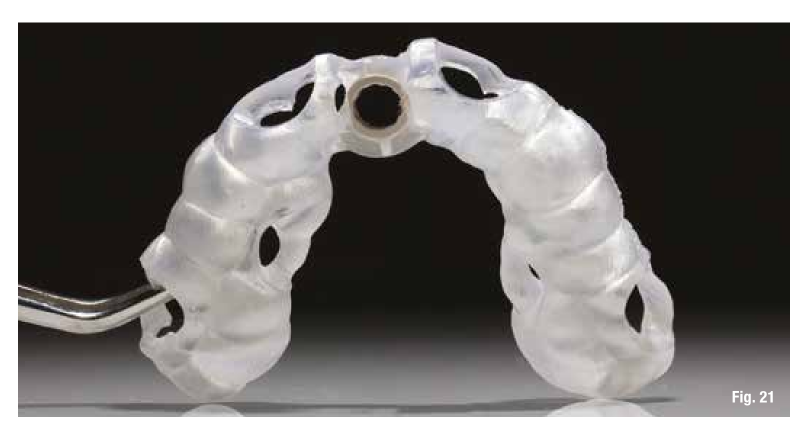
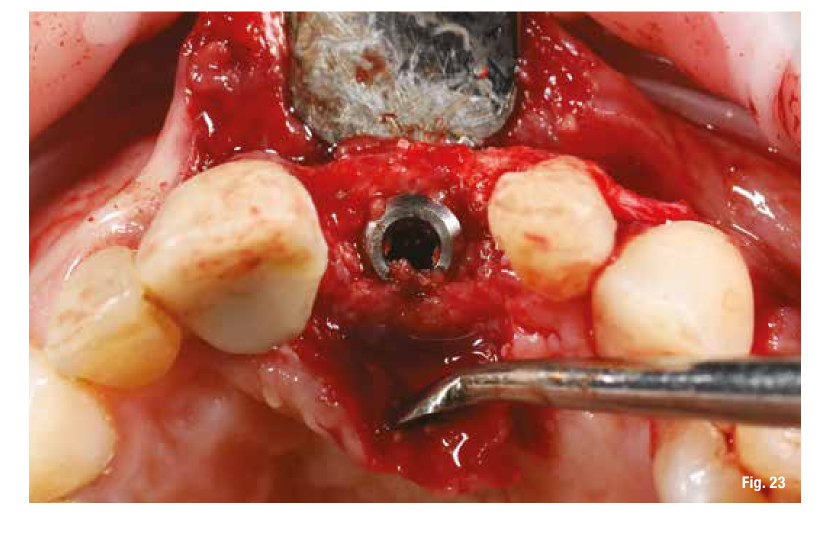
Видалення решітки, яке відбулося через 6 місяців, у цих випадках є дуже простим і виконується шляхом створення важільного ефекту в точках різання, передбачених у решітці, які відокремлюють вестибулярну частину від палатальної (Рис. 19). Після видалення двох частин решітки ми перевіряємо обсяг і якість регенерації (Рис. 20), а потім продовжуємо підготовку імплантаційного ложа, використовуючи хірургічну шаблон (Рис. 21, 22). У місцях з високою естетичною цінністю та з імплантом між двома природними елементами глибина імплантації є основоположною, і, якщо вона запланована до хірургії, це дозволяє нам бути більш передбачуваними (Рис. 23).


Використання хірургічного шаблону гарантує правильну глибину вставки, тому ми обираємо імплантат з продуктивною формою спіралей (TLX Straumann). Вставивши імплантат і перевіривши момент вставки, ми також розміщуємо миттєве відновлення, щоб відразу вплинути на пері-імплантні тканини (Рис. 24-26).



Висновки
Керована регенерація кістки є усталеною та добре задокументованою процедурою для виправлення горизонтального та/або вертикального дефіциту кістки. Ця техніка має дуже високий рівень успіху. Використання технік GBR за допомогою титанових решіток на замовлення Yxoss CBR виявилося ефективним хірургічним рішенням, особливо для вертикальних та комбінованих дефектів. Управління м'якими тканинами для забезпечення достатнього покриття залишається одним з найкритичніших етапів цієї техніки. Витяг решітки не призводить до повної втрати трансплантату. Представлений клінічний випадок демонструє, що решітка Yxoss CBR може забезпечити відмінну регенерацію кістки, з перевагою прискорення та оптимізації хірургічної процедури. Ці передумови дозволяють імплантацію, керовану протезуванням, забезпечуючи основи для функціонально та естетично адекватної імпланто-протезної реабілітації.
Санто Гароккіо, Філіппо Томареллі, Мауріціо Де Франческо, Джузеппе Марано
Бібліографія:
- Moraschini V., Poubel LA., Ferreira VF., Barboza ES.. Оцінка виживаності та успішності дентальних імплантатів, про які повідомляється в довгострокових дослідженнях з періодом спостереження не менше 10 років: систематичний огляд. Int J Oral Maxillofac Surg. 2015;44(3):377–88. PubMed PMID:25467739.
- Al-Nawas B., Kammerer PW., Morbach T., Ladwein C., Wegener J., Wagner W.. Десятирічне ретроспективне дослідження TiOblast дентального імплантату. Clin Implant Dent Relat Res. 2012;14(1):127–34. PubMed PMID: 20156231.
- Schiegnitz E., Al-Nawas B., Tegner A., Sagheb K., Berres M., Kammerer PW., та ін. Клінічний та радіологічний довгостроковий результат системи імплантатів з конічною формою з особливим акцентом на вплив процедур збільшення. Clin Implant Dent Relat Res. 2016;18(4):810–20. PubMed PMID: 25810365.
- Jung RE., Fenner N, Hammerle CHF., Zitzmann NU.. Довгостроковий результат імплантатів, встановлених з керованою регенерацією кістки (GBR) з використанням резорбованих та нерезорбованих мембран через 12–14 років. Clin. Oral Impl. Res. 24, 2013, 1065–1073.
- Setiawan Budihardja A., Mücke T.. “Управління кісткою в дентальній імплантології”.
- Cucchi та ін. Клінічні та об'ємні результати після вертикального збільшення гребеня з використанням комп'ютерного проектування/комп'ютерного виробництва (CAD/CAM) індивідуальних титанових сіток: пілотне дослідження. BMC Oral Health (2020) 20:219.
- De Santis D., Cucchi A., Rigoni G., Longhi C.. Короткі імплантати з окисленою поверхнею в задніх ділянках атрофічних щелеп: результати 3-5 років багатопрофільного дослідження. Clin Implant Dent Relat Res. 2015;17(3):442–52.
- Malchiodi L., Ghensi P., Cucchi A., Pieroni S., Bertossi D.. Умови навколо імплантатів з пористою поверхнею (SPS). Перспективне когортне дослідження на 36 місяців. Clin Oral Implants Res.2015;26(2):212–9.
- Rocchietta I., Ferrantino L., Simion M.. Вертикальне збільшення гребеня в естетичній зоні. Periodontol. 2018;77(1):241–55.
- Cucchi A., Chierico A., Fontana F., Mazzocco F., Cinquegrana C., Belleggia F., Rossetti P., Soardi CM., Todisco M., Luongo R., Signorini L., Ronda M., Pistilli R. Заяви та рекомендації щодо керованої регенерації кістки: звіт про консенсус симпозіуму з керованої регенерації кістки, що відбувся в Болоньї, 15-16 жовтня 2016 року. Implant Dent. 2019;28(4):388–99.
- Buser D., Bornstein MM., Weber HP., Grutter L., Schmid B., Belser UC. Раннє встановлення імплантатів з одночасною керованою регенерацією кістки після видалення одного зуба в естетичній зоні. Перехресне, ретроспективне дослідження на 45 суб'єктах з періодом спостереження 2-4 роки. J Periodontol. 2008;79:1773–81.
- Hammerle CH., Lang NP.. Одноетапна хірургія, що поєднує установку трансмукозного імплантату з керованою регенерацією кістки та біорозкладними матеріалами. Clin Oral Implants Res. 2001;12:9–18.
- Hurzeler MB., Strub JR.. Керована регенерація кістки навколо відкритих імплантатів. Новий біорозкладний пристрій та біорозкладні мембранні шпильки. Pract Periodontics Aesthet Dent. 1995;7:37–47.
- Buser D., Dahlin C.. Кісткові трансплантати та матеріали заміщення кістки. У: Buser D, редактор. Керована регенерація кістки в імплантології. 2-е вид. Чикаго, IL: Quintessence; 2009. с. 71–96.
- Rasia-dal Polo M., Poli PP., Rancitelli D., Beretta M., Maiorana C.. Реконструкція альвеолярного гребеня з титановими сітками: систематичний огляд літератури. Med Oral Patol Oral Cir Bucal. 2014 Nov;19(6):e639–46.
- Maiorana C., Santoro F., Rabagliati M., Salina S.. Оцінка використання іліакальної губчастої кістки та неорганічної бичачої кістки в реконструкції атрофічної верхньої щелепи з титановою сіткою: клінічне та гістологічне дослідження. Int J Oral Maxillofac Implants. 2001 May–Jun;16(3):427–32.
- Artzi Z., Dayan D., Alpern Y., Nemcovsky CE.. Вертикальне збільшення гребеня з використанням ксеногенних матеріалів, підтримуваних налаштованою титановою сіткою: клініко-гистопатологічне та гістохімічне дослідження. Int J Oral Maxillofac Implants. 2003 May–Jun;18(3):440–6.
- Troeltzsch M., Troeltzsch M., Kauffmann P., Gruber R., Brockmeyer P., Moser N., Rau A., Schliephake H.. Клінічна ефективність матеріалів для трансплантації в збільшенні альвеолярного гребеня: систематичний огляд. J Craniomaxillofac Surg. 2016 Oct;44(10):1618–29.
- Sumida T., Otawa N., Kamata YU., Kamakura S., Mtsushita T., Kitagaki H., Mori S., Sasaki K., Fujibayashi S., Takemoto M., Yamaguchi A., Sohmura T., Nakamura T., Mori Y.. Індивідуальні титанові пристрої як мембрани для збільшення кістки в лікуванні імплантатами: клінічне застосування та порівняння з традиційною титановою сіткою. J Craniomaxillofac Surg. 2015 Dec;43(10):2183–8.
- Sagheb K., Schiegnitz E., Moergel M., Walter C., Al-Nawas B., Wagner W.. Клінічний результат збільшення альвеолярного гребеня з індивідуальною титановою сіткою, виготовленою за допомогою CAD-CAM. Int J Implant Dent. 2017 Dec;3(1):36. doi: 10.1186/ s40729-017-0097-z.
- Seiler M., Peetz M., Hartmann A., Witkowski R.. Індивідуальні титанові каркаси, виготовлені за допомогою CAD/CAM, для збільшення альвеолярної кістки: ретроспективний аналіз подій декомпенсації у зв'язку з демографічними та хірургічними параметрами. J Oral Science Rehabilitation. 2018 Mar;4(1):38–46.
- Chiapasco M., Casentini P., Tommasato G., Dellavia C., Del Fabbro M.. Індивідуальні титанові сітки CAD/CAM для керованої регенерації кістки при важких дефектах альвеолярного гребеня: попередні результати ретроспективного клінічного дослідження на людях. Clin Oral Implants Res. 2021. Apr;32(4):498-510.
- Dellavia C., Canciani E., Pellegrini G., Tommasato G., Graziano D., Chiapasco M.. Гістологічна оцінка тканини щелепної кістки після керованої регенерації кістки з використанням індивідуальної титанової сітки, виготовленої за допомогою комп'ютерного проектування/комп'ютерного виробництва у людей: когортне дослідження. Clin Implant Dent Relat Res. 2021;1–12.
- Garocchio S., імплантати Італія №2, 2021