
Цифровий робочий процес у реабілітації імплант-протезування в естетично важливих ділянках: від літератури до клініки
Машинний переклад
Оригінальна стаття написана мовою IT (посилання для прочитання) .
Сьогодні цифровий робочий процес відіграє все більш важливу роль в стоматології. Перевага комп'ютерно-асистованої імплантації (CAI, Computer Aided Implantology) полягає в розміщенні імплантатів за допомогою хірургічного шаблону, спроектованого та виготовленого за технологією CAD/CAM; таке розміщення, протезно-орієнтоване, імплантатів досягається за допомогою програмного забезпечення для віртуального планування імплантації. У реабілітаціях імпланто-протезування передніх секторів за допомогою комп'ютерно-асистованої хірургії можливо правильно розмістити імплантати для досягнення оптимального естетичного результату. Метою цього клінічного випадку є показати реабілітацію верхнього центрального різця шляхом негайного комп'ютерно-асистованого розміщення імплантату з протоколом негайного навантаження протеза.
Вступ
Реабілітація імпланто-протезування фронтальних секторів з високою естетичною цінністю є викликом, з яким клініцист повинен зіткнутися, знаючи досконало різні терапевтичні варіанти, що є в його розпорядженні, методики, які походять з суворого та уважного вивчення наукової літератури.
Передімплантаційний аналіз естетичних параметрів EIND1 дозволяє виявити критичні моменти випадку та оптимізувати його реалізацію, визначаючи тип імплантаційної хірургії та естетичний результат залежно від хірургічного таймінгу (клас 1, 2, 3, 4). 4D позиціонування, описане вже в 2007 році групою Салами, підкреслює, що клінічний успіх залежить не лише від ідеального тривимірного позиціонування імплантату в кістці, але й від правильної управлінської стратегії профілів жорстких і м'яких тканин, які дуже часто потребують збільшень або корекцій, а також від правильного дизайну імплантату та протеза.
Цифровий аналіз, що складається з оптичного внутрішньоротового зліпка на діагностичному етапі, аналогової або цифрової діагностичної воскової моделі, передопераційної CBCT та зіставлення всієї цієї інформації в програмному забезпеченні комп'ютерно-асистованої хірургії, дозволяє максимально ефективно використовувати зібрану інформацію та виконувати протезно-орієнтовану хірургію.
Матеріали та методи
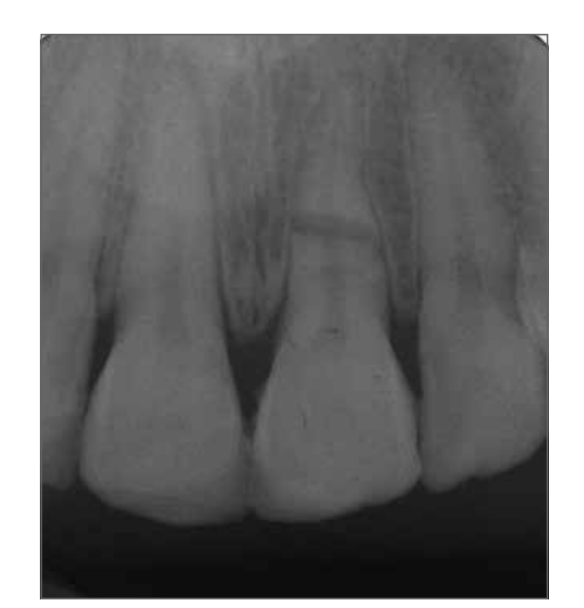
Пацієнтка МС, 24 роки, звернулася до нас в екстреному порядку через наслідки дорожньо-транспортної пригоди. Під час клінічного обстеження поза та всередині ротової порожнини спостерігалися розрив верхньої губи, частковий коронковий перелом зубів 1.2, 1.1 та 2.1, а також горизонтальний перелом на рівні середньої третини кореня зуба 2.1, що було підтверджено періапікальною рентгенограмою, виконаною з центратором Рінна (Рис. 1-3).


Зубні елементи 1.1 та 1.2 були відновлені (з відсутністю життєздатності пульпи, яку потрібно перевірити знову через 3 та 5 місяців), тоді як зубний елемент 2.1, який не підлягав відновленню, потребував видалення.
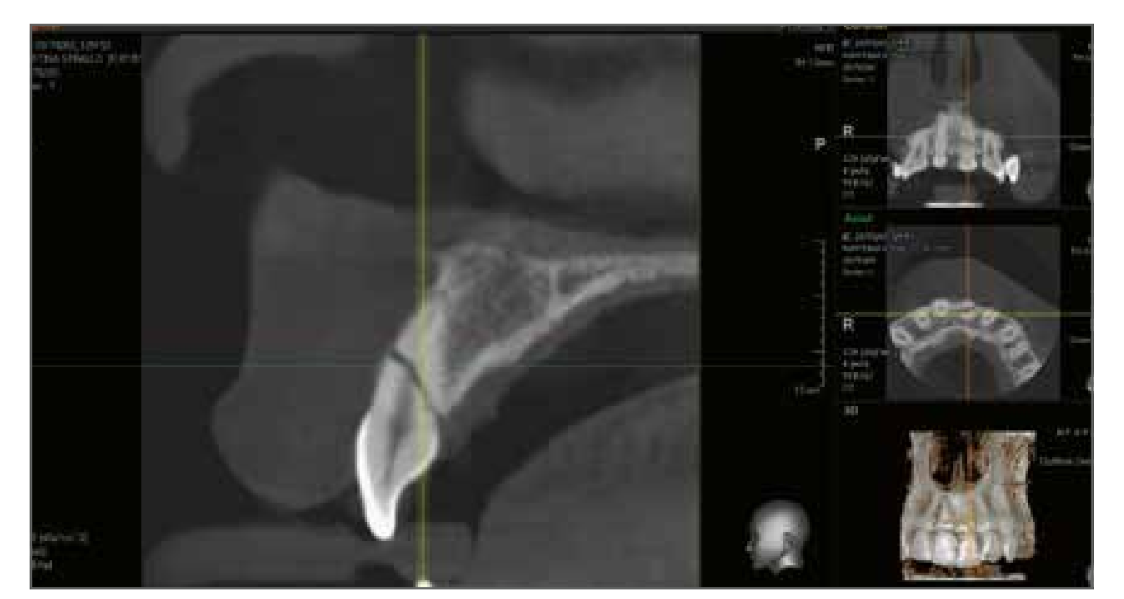
Після ретельної діагностичної оцінки з клінічним обстеженням, яке виявило відсутність пародонтального зондажу, що могло б свідчити про перелом вестибулярної кісткової кори, та з тривимірним рентгенівським обстеженням (Рис. 4), яке показало цілісність кори, було вирішено, за згодою пацієнтки, провести негайну імпланто-протезну реабілітацію за допомогою комп'ютерно-асистованої хірургії з негайним навантаженням. Повний фотосет, разом з клінічними та рентгенівськими обстеженнями, виявив критичні моменти випадку: молода пацієнтка, верхній центральний різець, надзвичайно високі естетичні вимоги, тонкий і фестончастий пародонтальний біотип, кореневий перелом між середньою та апікальною третинами.
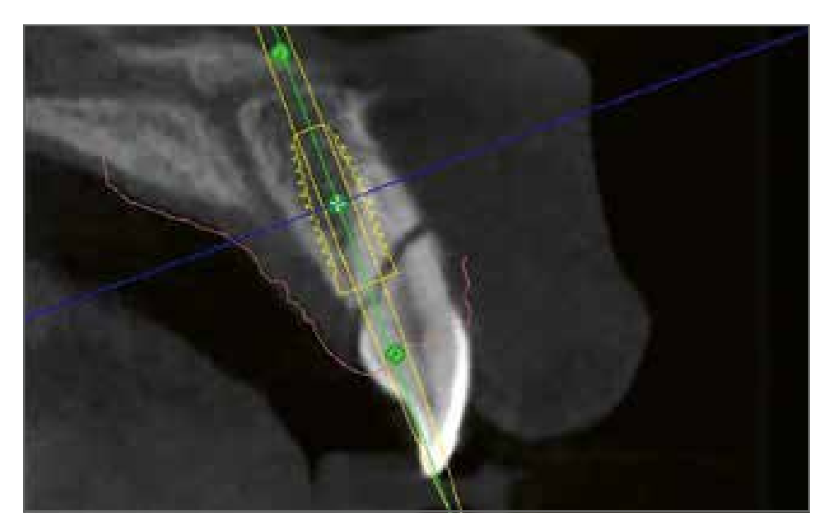
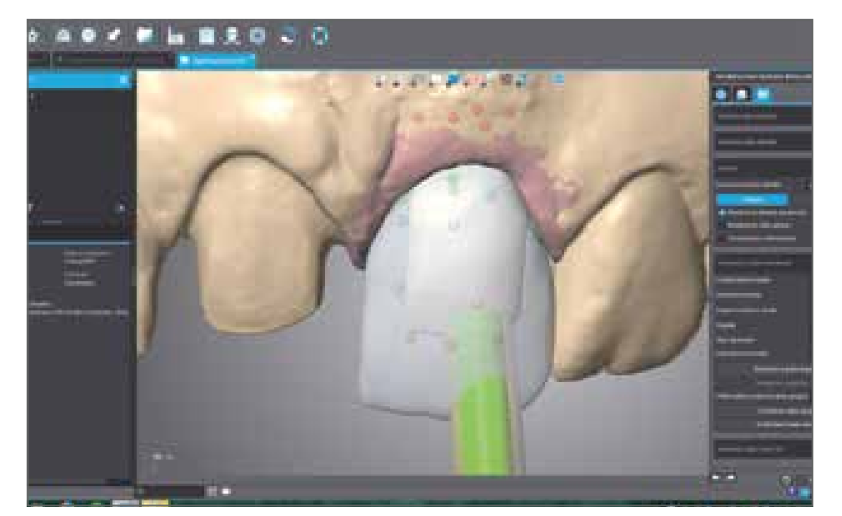
Було знято два цифрові відбитки щелеп, виконано діагностичне воскове моделювання на елементі 2.1 та проведено CBCT з підтримкою оклюзійної реєстрації Navibite (Biomax, Віченца), які разом з 2 файлами STL завантажувалися в програмне забезпечення Navimax для планування видалення та миттєвого встановлення імплантату відносно кісткового гребеня, кісткового краю сусіднього різця та діагностичного воскового моделювання (Рис. 5). Відповідно до даних, наведених у літературі, було заплановано встановлення імплантату Biomet 3I T3 (Biomet, Палм-Біч-Гарденс, Флорида, США) з інтегрованим платформним перемиканням 4/3 x 13 мм, розташованого на 1,5 мм нижче вестибулярного краю гребеня, який слід зберегти недоторканим під час видалення зуба. Аналіз у Navimax дозволяв спостерігати, як правильне розташування імплантату в трьох вимірах простору виявляло на імплантоцентричному зображенні наявність кістки на 360°, як первинна стабільність імплантату могла бути досягнута також у апікальній частині зубної альвеоли та як вісь протезного виходу дозволяла управляти миттєвим навантаженням з використанням вкручуваного тимчасового протезу. Після підтвердження хірургічного планування файл надсилався до виробничого центру для виготовлення хірургічної шаблону Navident з опорою на зуби (Рис. 6).

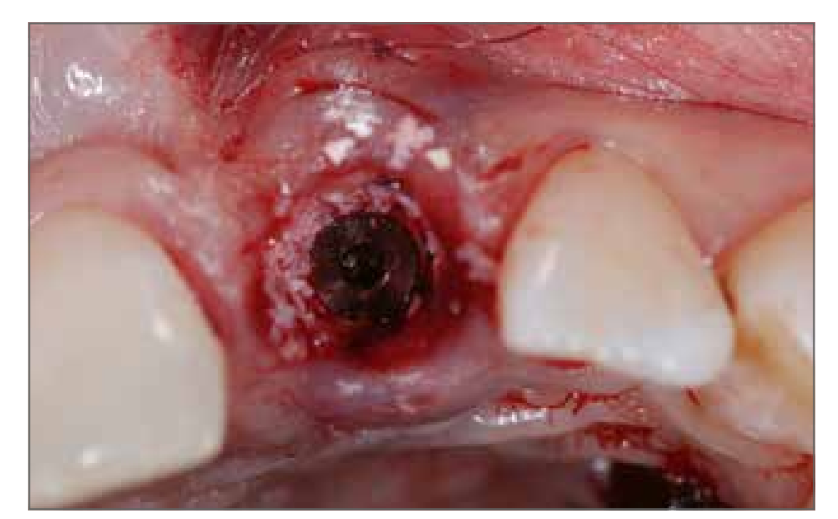
На момент хірургічного втручання (3 дні після інциденту), після відповідної антибіотикопрофілактики (2 г амоксициліну та клавуланової кислоти за 1 годину до втручання) та після плесикової анестезії з артикаїном 1:100.000, без розрізу мезіальних та дистальних сосочків, без травматично видалялися зубний елемент 2.1 (Рис. 7) за допомогою п'єзоелектричних інструментів, зберігаючи вестибулярну кортикаль (необхідну для управління негайним післявидаленням). Після встановлення хірургічної шаблону, готувався імплантаційний сайт за допомогою хірургічного набору Navigator з технікою підготовки та було встановлено, як заплановано, імплантат Biomet 3I T3 4/3 x 13 мм (Рис. 8); момент вставки перевищував 70 N/cm, а частота резонансу, виміряна з Osstel, становила 68 ISQ (Рис. 9). Періімплантаційний проміжок управлявся, відповідно до даних, наявних у літературі5, з використанням депротенізованого кісткового порошку великої рогатої худоби (Bio-Oss гранули, Geistlich Biomaterials, Thiene) для протидії резорбції вестибулярної кістки. Як було проаналізовано на діагностичному етапі, пацієнтка мала тонкий та фестончастий біотип, що вимагало збільшення та стабілізації м'яких тканин з одного боку за допомогою імплантату з платформним перемиканням, щоб мати більше місця для досягнення стабільності м'яких тканин, з іншого боку, з використанням сполучної тканини, вставленої в блістер з частковою вестибулярною товщиною. Забір був виконаний в піднебінній області, після анестезії навколишньої зони з артикаїном 1:100.000, з прямокутним епітеліально-з'єднувальним розрізом товщиною 1,5 мм, висотою близько 4 мм та довжиною, що дорівнює зоні, що підлягає обробці, близько 10 мм (Рис. 10).



Після накладення швів на донорське місце, було здійснено дисепітелізацію трансплантату, залишивши сполучнотканинний шар товщиною приблизно 1,2 мм, який був розміщений, після часткового вестибулярного розрізу в елементі 2.1, на 1 мм вище кісткового гребеня і зашитий розсмоктувальним швом Vicryl 6-0, таким чином, щоб отримати товщину вестибулярного клаптя між 2,5 і 3 мм, як зазначено в роботах Zucchelli та співавт.6 (Рис. 11). Тимчасовий протез, отриманий з діагностичної воскової моделі, був потім розміщений і перероблений в роті за допомогою протезної шаблону для повторного позиціонування. Підясенний профіль тимчасового протезу був збережений увігнутим без компресії вестибулярних тканин, щоб залишити простір для зрілості м’яких тканин. Місцеві та дистальні контактні точки були оброблені відповідно до вказівок Tarnow та співавт.7,8 для досягнення повної реформації міжзубних сосочків (Рис. 12). Крім того, тимчасовий протез був звільнений у контактах в центральному, протрузійному та латеральному положеннях. Пацієнтка була виписана з підтримуючою медикаментозною терапією та була запрошена на клінічні та артикуляційні контролі через 2 тижні (видалення шва), 4, 8, 12 та 16 тижнів, спостерігаючи за зрілістю м’яких тканин та рентгенівським загоєнням кістки.

Через 4 місяці, при збереженні відсутності життєздатності елемента 1.1, була проведена канальна терапія, реконструкція з використанням скловолоконного штифта та встановлення тимчасової коронки з смоли.
Видалення тимчасової коронки, закріпленої на імплантаті, через 4 місяці після хірургічного втручання дозволило виявити ідеальну інтеграцію сполучної тканини та васкуляризацію ділянки з циркулярними та перпендикулярними сполучними волокнами (Рис. 13); новий рівень частоти резонансу зріс до 80 ISQ.

Фіналізація випадку передбачала використання методики цифрового зняття відбитків з оптичним внутрішньоротовим сканером Carestream 3600 (Carestream Health, Рочестер, Нью-Йорк, США). Згідно з правильним цифровим протоколом, було отримано оптичний відбиток верхньої щелепи з встановленими тимчасовими коронками, екстраоральний відбиток окремих тимчасових коронок, відбиток природного зуба, належним чином підготовленого з використанням ретракційного шнура Ultrapack 00 (Ultradent Products Inc., Солт-Лейк-Сіті, Юта, США) та підготовки з модифікованим шанфером, відбиток трансмукозного шляху, отриманого з імплантаційного сайту, та відбиток позиціонування імплантату з використанням скан-боді (Рис. 14,15). Нарешті, було отримано відбиток антагоністичної щелепи та перевірка оклюзійної реєстрації.


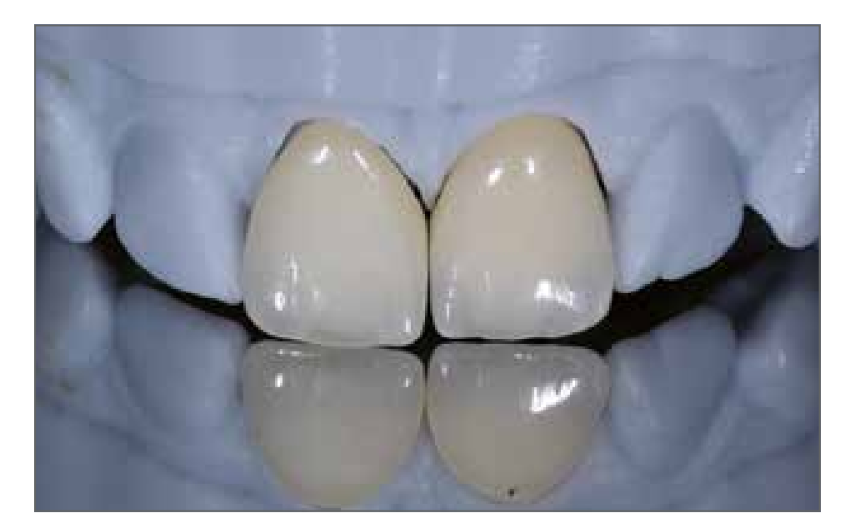
Лабораторні етапи, також виконані з майже повністю цифровим потоком, передбачали виготовлення імплантаційного стовпа з цирконію з технікою склеювання, з конвексним підясенним профілем, та 2 коронки з цирконієвої кераміки, які були нашаровані: звідси виникла необхідність мати також робочу модель з поліуретану, яка дозволила правильні нашарування кераміки для досягнення відмінної естетики, що могла б задовольнити пацієнта, клініциста та зубного техніка (Рис. 16-18). Умови м'яких тканин на елементі 2.1 виявилися ідеальними і дозволили, після затягування стовпа з цирконію до 25 Н/см та адгезивного цементування двох корон, досягти оптимальної естетики та маскування двох центральних різців (Рис. 19-22).


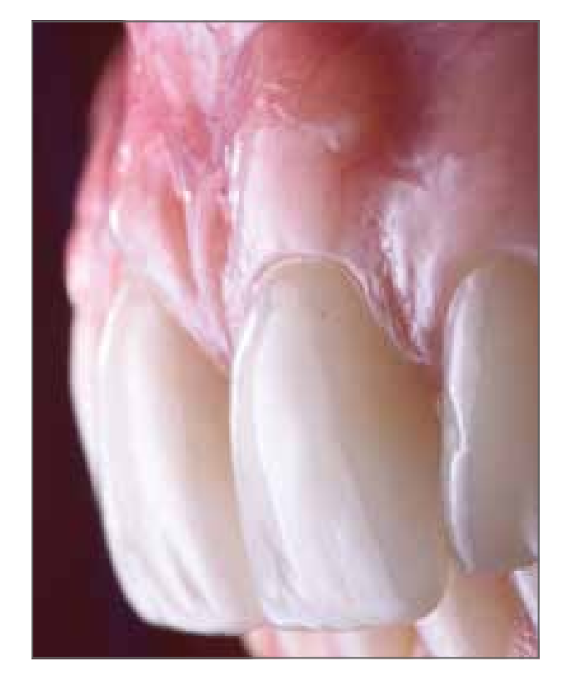


Рентгенівські обстеження в двох і трьох вимірах підтверджують отриманий результат (Рис. 23,24). Контроль через 24 місяці показав оптимальний естетичний результат з стабілізацією твердих і м'яких тканин (Рис. 24).


Обговорення
Можливість віртуального проектування імплантації зубних імплантів та їх розміщення в точній тривимірній позиції всередині альвеолярної кістки за допомогою відповідно оброблених або надрукованих на 3D-принтері хірургічних шаблонів вже давно є надійною та передбачуваною клінічною реальністю. Насправді, керована хірургія вважається успішною клінічною процедурою вже понад 10 років, про що свідчать численні клінічні роботи та систематичні огляди літератури.
Крім того, впровадження технологій для отримання цифрових зображень повністю змінило робочий процес. По-перше, впровадження конусно-променевої комп'ютерної томографії (CBCT), яка дозволяє отримувати 3D інформацію про кісткову анатомію з низькою дозою радіації для пацієнта та високою якістю зображень. По-друге, впровадження все більш точних та ефективних інтраоральних оптичних сканерів стало ще однією еволюцією в техніках отримання зображень для хірургічного планування. Адже завдяки таким пристроям можна просто, точно та точково отримувати всі необхідні дані про тверді та м'які тканини за допомогою простого світлового променя. Крім того, у разі виявлення дефектів або недоліків на зображенні, можна повторно зняти лише невелику ділянку, де було виявлено помилку, без необхідності повторно знімати весь відбиток, як це відбувається при аналоговому відбитку.
Ці нові технології дозволили, обробляючи дані та інформацію, отримані за допомогою спеціалізованого програмного забезпечення, покращити передопераційне планування, симулюючи як хірургічну, так і протезну стадії, але також дозволили виготовлення хірургічної шаблони на основі зубів виробничим центром.
Очевидно, що є безліч переваг переходу від аналогового робочого процесу до цифрового, серед яких: краща діагностика та планування лікування, з можливістю детально вивчати та планувати терапії в 3D, будь то протезні, хірургічні чи ортодонтичні; контроль якості виробничих процесів, зі стандартизацією на оптимальних рівнях протезних реставрацій з високоестетичних матеріалів; у хірургії підвищується безпека завдяки керованому розташуванню імплантатів (можливість повністю цифрового робочого процесу) та використанню ін grafts та титанових сіток на замовлення, персоналізованих під дефект пацієнта; зниження витрат, пов'язаних не лише з виробничими процесами, але й з витратними матеріалами (зменшення потреби в традиційних матеріалах для зняття відбитків, відсутність витрат на доставку, оскільки файли надсилаються електронним шляхом); скорочення часу лікування, оскільки значно зменшується кількість прийомів, що економить час для лікаря та пацієнта; менший стрес для пацієнта під час процедур зняття відбитків за допомогою інтраорального сканера; сприйняття високої якості з боку пацієнта, з яким можна безпосередньо спілкуватися, показуючи зображення 3D високої якості різних хірургічних та протезних етапів, що дозволяє йому легше приймати витрати, пов'язані з навіть складними лікуваннями.
Незважаючи на численні переваги, на сьогоднішній день ще не існує широкого впровадження цифрового робочого процесу, що, ймовірно, пов'язано з наступними причинами: очевидна складність протоколів та їх застосування; крива навчання; витрати на запуск, пов'язані з придбанням обладнання та щорічним оновленням програмного забезпечення; витрати на окремі пристрої (дими та спеціалізовані хірургічні набори).
Проте, з появою на ринку все більшої кількості компаній, що спеціалізуються в цифровій сфері, спостерігається збільшення пропозиції та конкуренції, що призводить до значного зниження цін. Внаслідок цього як програмне забезпечення, так і цілі робочі процеси значно спростилися, що зробило їх більш доступними для клініцистів.
Висновки
Реабілітація імплантно-протезного лікування центрального різця молодої пацієнтки є великою викликом та зобов'язанням для клініциста: сучасні цифрові технології, які починаються з тривимірного обстеження щелепних кісток та зубних дуг, з цифрового аналізу усмішки з wax-up і закінчуються реалізацією комп'ютерно керованої імплантаційної хірургії з миттєвою протезуванням, дозволяють оптимізувати робочий процес і досягти, відповідно до даних, представлених у науковій літературі, функціональних та естетичних результатів.
Філіппо Томареллі, Джузеппе Марано, Мауріціо Де Франческо, Джорджо Серафіні
Бібліографія
- Дурсун Е, Лін ГХ, Тахері С, Чу СД, Ван ХЛ, Тезюм ТФ. Порівняння естетичних характеристик природного зуба та реставрації після імплантації в естетичній зоні: ретроспективне спостереження протягом 12 місяців. Int J Oral Maxillofac Implants. 2018 Лип/Сер;33(4):919-928.
- Фунато А, Салама МА, Ішікава Т, Гарбер ДА, Салама Х. Час, позиціонування та послідовні етапи в естетичній імплантаційній терапії: чотиривимірна перспектива. Int J Periodontics Restorative Dent. 2007 Серп;27(4):313-23.
- Грундер У. Зміни ширини кристального гребеня при встановленні імплантів під час видалення зубів з і без збільшення м'яких тканин після періоду загоєння 6 місяців: звіт про 24 послідовні випадки. Int J Periodontics Restorative Dent. 2011 Лют;31(1):9-17.
- Чен СТ, Бусер Д. Естетичні результати після негайного та раннього встановлення імплантів у передній щелепі - систематичний огляд. Int J Oral Maxillofac Implants. 2014;29 Suppl:186-215.
- Чу СД, Салама МА, Гарбер ДА, Салама Х, Сарначіаро ГО, Сарначіаро Е, Готта СЛ, Рейнольдс МА, Сайто Х, Тарнов ДП. Встановлення імплантів без клаптя після видалення зуба, Частина 2: Вплив кісткової пластики та тимчасової реставрації на висоту та товщину м'яких тканин навколо імплантів - ретроспективне дослідження. Int J Periodontics Restorative Dent. 2015 Лис-Груд;35(6):803-9.
- Цуккелі Г, Горі Г, Меле М, Стефаніні М, Маццотті Ч, Марзадорі М, Монтебуньолі Л, Де Санктіс М. Некаріозні шийкові ураження, пов'язані з рецесією ясен: процес прийняття рішень. J Periodontol. 2011 Груд;82(12):1713-24.
- Юнг РЕ, Хейтц-Мейфілд 2, Шварц Ф; Групи 2-ї Консенсусної зустрічі Фонду остеології. Доказова база знань про естетику та підтримку м'яких тканин навколо імплантів: Консенсусний звіт Фонду остеології Частина 3 - Естетика м'яких тканин навколо імплантів. Clin Oral Implants Res. 2018 Бер;29 Suppl 15:14-17.
- Тарнов Д, Еліан Н, Флетчер П, Фрум С, Магнер А, Чо СК, Салама М, Салама Х, Гарбер ДА. Вертикальна відстань від гребеня кістки до висоти міжпроксимальної папили між сусідніми імплантами. J Periodontol. 2003 Груд;74(12):1785-8.
- Тесторі Т, Робіоні М, Паренті А, Лунго Г, Розенфельд АЛ, Ганц СД, Манделаріс ГА, Дель Фаббро М. Оцінка точності та прецизійності нової системи керованої хірургії: багатопрофільне клінічне дослідження. Int J Periodontics Restorative Dent. 2014;34 Suppl 3:s59-69.
- Ван Асше Н, Веркруйссен М, Кук В, Тейгельс В, Якобс Р, Квірінен М. Точність комп'ютерного планування імплантації. Clin Oral Implants Res. 2012 Жов;23 Suppl 6:112-23.
- Дас М, Ассаф А, Дада К, Макзуме Ж. Комп'ютерно-керована імплантаційна хірургія в свіжих лунках після видалення зубів та негайне навантаження повної реставрації: дослідження з 2-річним спостереженням за 14 послідовно лікуваними пацієнтами. Int J Dent. 2015;2015:824127.
- Д’Гейз Ж, Ван Де Вельде Т, Коміяма А, Хультін М, Де Бруїн Х. Точність і ускладнення використання комп'ютерно спроектованих стереолітографічних хірургічних направляючих для оральної реабілітації за допомогою зубних імплантів: огляд літератури. Clin Implant Dent Relat Res. 2012 Черв;14(3):321-35.
- Ганц СД. Трьохвимірна візуалізація та керована хірургія для зубних імплантів. Dent Clin North Am. 2015 Квіт;59(2):265-90.
- Аль-Окші А, Лінд Х, Сале Х, Гуннарссон М, Рохлін М. Ефективна доза конусно-променевої КТ (CBCT) лицьового скелета: систематичний огляд. Br J Radiol. 2015 Січ;88(1045):20140658.
- Давуд А, Браун Дж, Саурет-Джексон В, Пуркаяста С. Оптимізація експозиції конусно-променевої КТ для передопераційної оцінки місця імплантації. Dentomaxillofac Radiol. 2012 Січ;41(1):70-4.
- Циммерманн М, Мель А, Морманн ВХ, Рейх С. Системи внутрішньоротового сканування - сучасний огляд. Int J Comput Dent. 2015;18(2):101-29.
- Тінг-Шу С, Цзян С. Техніка внутрішньоротового цифрового зняття відбитків: огляд. J Prosthodont. 2015 Черв;24(4):313-21.
- Юзбашіоглу Е, Курт Х, Турунч Р, Біляр Х. Порівняння цифрових та традиційних технік зняття відбитків: оцінка сприйняття пацієнтів, комфорту лікування, ефективності та клінічних результатів. BMC Oral Health. 2014 30 Січ;14:10.
- Патцельт СБ, Лампрінос Ч, Штампф С, Атт В. Часова ефективність внутрішньоротових сканерів: порівняльне in vitro дослідження. J Am Dent Assoc. 2014 Черв;145(6):542-51.