
Діагностичне значення цифрової об'ємної томографії у виявленні вестибулярної кореневої перфорації: клінічний випадок
Машинний переклад
Оригінальна стаття написана мовою ES (посилання для прочитання) .
Резюме
Досягнення успіху в ендодонтії пов'язане з точним діагнозом; встановлення діагностичної гіпотези, основаної лише на періапікальних рентгенограмах, є викликом для всіх спеціальностей стоматології. Повна та динамічна візуалізація тривимірних структур, доступна з допомогою цифрової об'ємної комп'ютерної томографії (КТ), сприяє точному визначенню проблеми та плануванню лікування.
Метою цього клінічного випадку є представлення реального клінічного погляду на необхідність оцінки анатомічних структур у трьох вимірах, після ендодонтичного невдачі, пов'язаної з вестибулярною кореневою перфорацією центрального верхнього різця, яка не могла бути виявлена на основі періапікальних рентгенограм. Пацієнт був прооперований за одну зустріч, і перфорація була хірургічно закрита за допомогою MTA. Після року спостереження було зафіксовано відсутність клінічної симптоматики.
У випадках перфорацій час є вирішальним фактором, тому найкращий момент для ремонту кореневої перфорації - це відразу після її виникнення, що мінімізує потенціал виникнення інфекції в місці перфорації.
Вступ
Необхідність оцінки зубних структур у трьох вимірах у ендодонтичній практиці дозволила нам діагностувати, планувати та вирішувати все більш складні випадки, пов'язані з іншими технологічними ресурсами. Звичайні рентгенівські знімки пропонують зображення у двох вимірах тривимірних тіл, що є недостатніми та обмежуючими в деяких випадках для виявлення багатьох визначальних деталей і знання елементів, які досі були приховані та/або важкі для сприйняття.
Ендодонтичне лікування пов'язане з випадковими, небажаними та непередбачуваними обставинами, які можуть призвести до невдачі лікування. Аварії під час ендодонтичної терапії можна визначити як ті нещасні випадки, які трапляються під час лікування; деякі з них через відсутність уваги, а інші через повну непередбачуваність. Серед процедурних аварій виділяються кореневі перфорації. Найбільшою ускладненням, викликаним перфорацією, є періодонтальне запалення та втрата кісткової вставки. У цьому сенсі їх виявлення, локалізація та терміновий ремонт є основними факторами для отримання задовільних результатів. З іншого боку, цей тип аварії вважається другою найпоширенішою причиною ендодонтичної невдачі.
Перфорації викликані різними причинами, включаючи труднощі у знаходженні каналів через аномальну морфологію, кальцифікацію пульпи, помилку під час доступу до пульпної камери, під час підготовки та формування кореневих каналів, при встановленні постів, під час повторних лікувань, а також внаслідок внутрішньої перфораційної резорбції до перірадикульних тканин.
У момент, коли відбувається перфорація, підтримуюча тканина (периодонтальна зв'язка та альвеолярна кістка) руйнується, в більшій чи меншій мірі залежно від калібру використаного інструменту, внаслідок чого виникає запальний процес змінної інтенсивності. Якщо лікування перфорації не проводиться, відбувається бактеріальне забруднення, яке визначає прогресію та еволюцію запального процесу, що, в свою чергу, призводить до більшого руйнування кістки в області перфорації, і поряд з цим цемент та сусідня дентин можуть мати ділянки резорбцій.
Тому в разі перфорацій час є вирішальним фактором; найкращий момент для ремонту перфорації кореня - це негайно після її виникнення, щоб зменшити потенціал появи інфекції в місці перфорації.
Ремонт перфорацій може бути виконаний хірургічним або нехірургічним способом; клінічна процедура буде залежати від локалізації перфорації. Фактори, що впливають на прогноз, це: розмір перфорації, пошкодження кістки та періодонту, час, що минув між перфорацією та ремонтом, здатність досягти герметичного ущільнення, а також чи є перфорація супраосною чи інфраосною.
У даному клінічному випадку розповідається про реальну важливість ТВД у діагностиці перфорації кореня вестибулярної, її лікування та хірургічного ущільнення з MTA Angelus (Angelus, Лондрина, PR, Бразилія) в одну сесію, отримуючи клінічний та рентгенографічний успіх після року еволюції.
Опис клінічного випадку
Пацієнтка жіночої статі, 29 років, направлена до клініки ендодонтії Госпіталю загального призначення армії Сан-Паулу (HGeSP). Під час анамнезу повідомляє про інтенсивний, пульсуючий біль та чутливість в передній ділянці, після того як була піддана лікуванню ендодонтії 3 тижні тому.
Клінічно при внутрішньоротовому огляді виявлено збільшення об'єму, почервоніння та набряклість слизової оболонки в періапікальній ділянці зуба 1.1. Термальні тести на пульпальну чутливість негативні, і пацієнтка відчуває інтенсивний біль при вертикальній перкусії. Пародонтальні зонди були в межах нормальних значень.
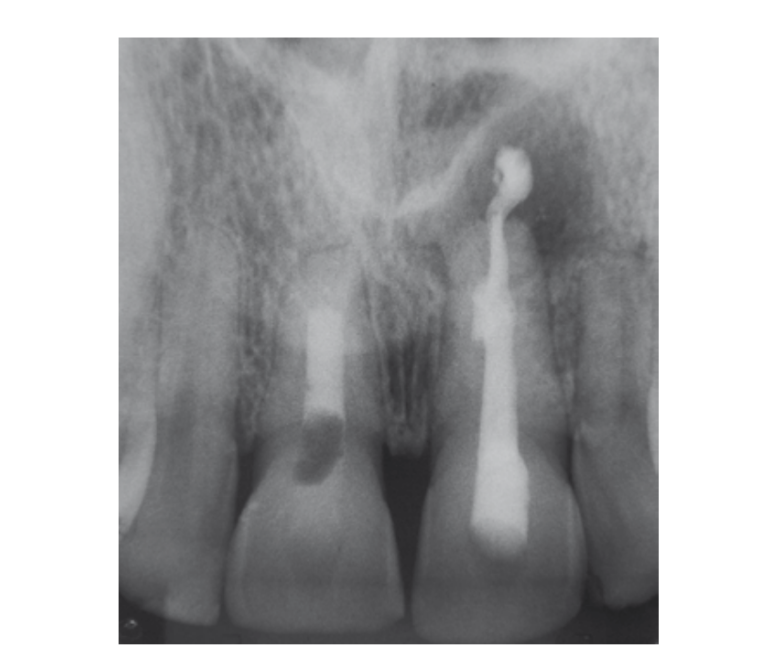
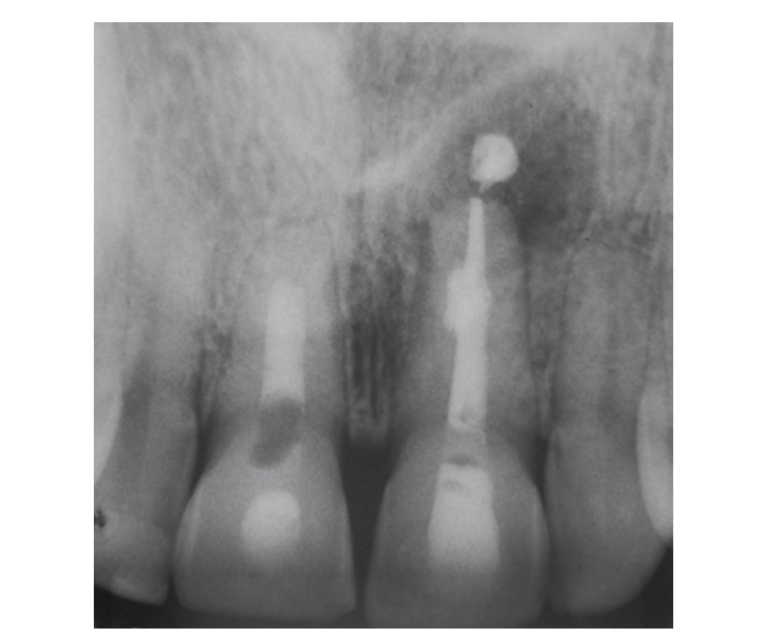
При рентгенографічному ретроальвеолярному огляді (Рис. 1) спостерігається ендодонтичне лікування в ідеальному стані, відсутність радіолucidних зон, що відповідають ураженню або втраті кістки в періапікальній або бічній ділянці. Також оцінюється зуб 2.1, який має пломбувальний матеріал в періапікальній ділянці. Клінічні знахідки не вказують на симптоматику, пов'язану з цим зубом.

На основі цього було запропоновано провести цифрову об'ємну томографію.
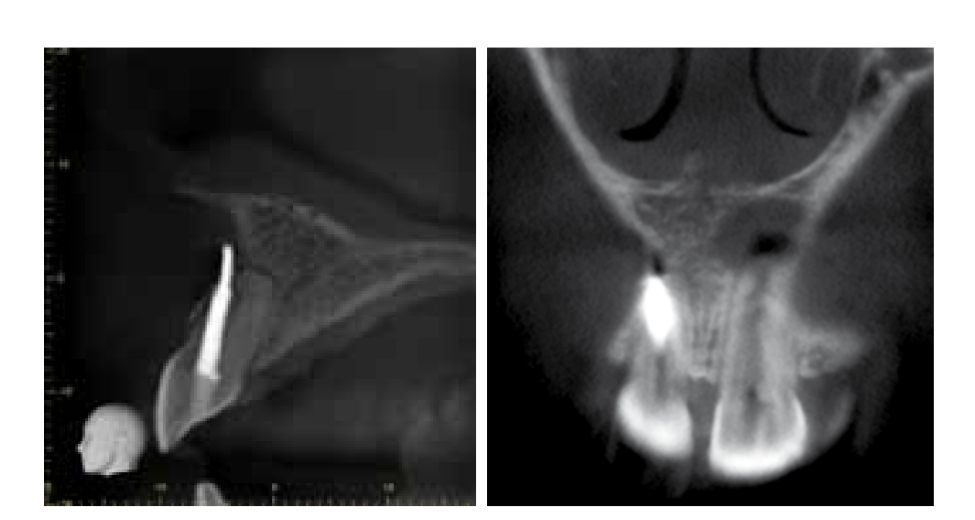
Було проведено оцінку цифрової комп'ютерної томографії високої роздільної здатності за допомогою програмного забезпечення для візуалізації зображень у 3D (i-Dixel 2.0 - One Volume Viewer, Accuitomo 80 - J. Morita Mfg. Corp., Кіото, Японія). На сагітальній та корональній проекціях було виявлено перфорацію з проходженням рентгенопрозорого матеріалу в палацитально-вестибулярному напрямку, що відповідає ендодонтичному матеріалу для пломбування. Також на площині об'ємної реконструкції спостерігається втрата кісткової тканини вестибулярної ділянки та перфорація вестибулярної кори (Рис. 2).
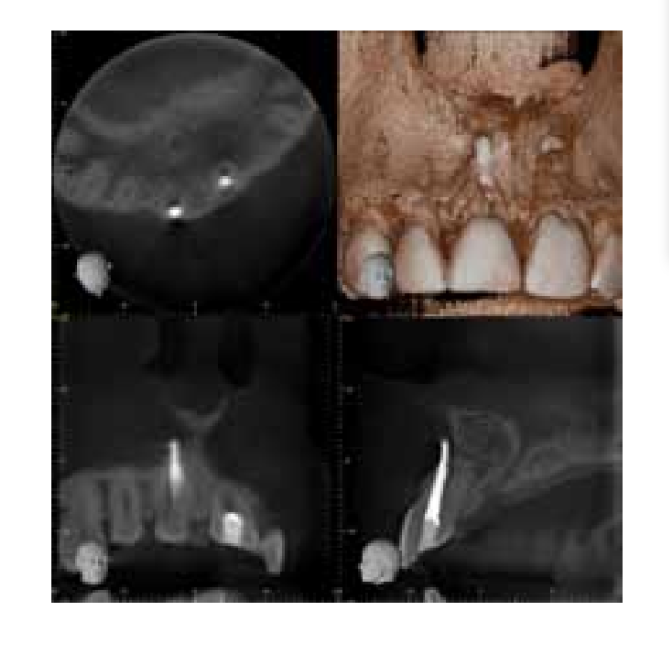
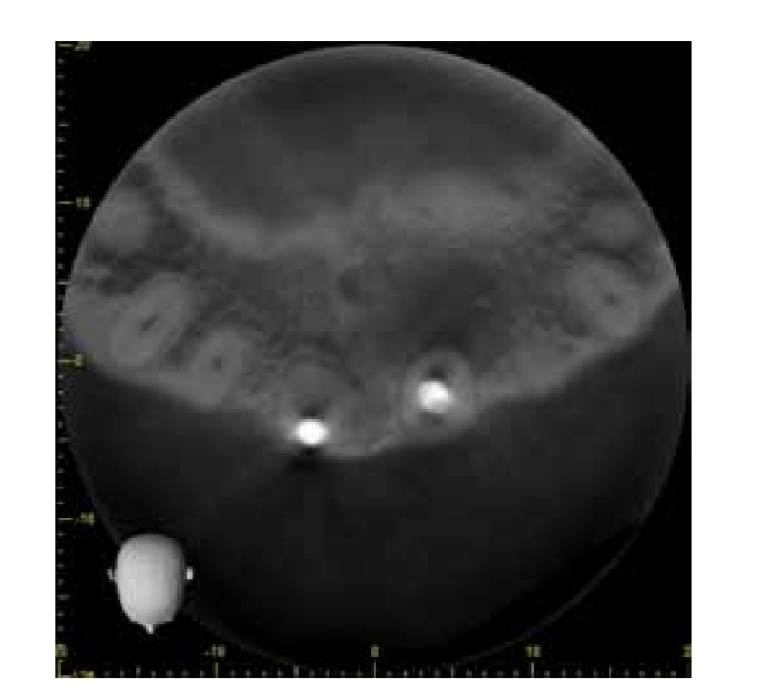
Оцінюючи аксіальний зріз (Рис. 3), було можливим спостерігати втрату центровки каналу та відсутність візуалізації його оригінального світла, що свідчить про кальцифікацію апікальної третини. На сагітальному та корональному зрізах ми можемо спостерігати точне розташування перфорації в середній третині та відхилення кореневої траєкторії в бік вестибулярної частини матеріалу пломбування (Рис. 4-5).
На основі інформації з високоякісних зображень було проведено ендодонтичне втручання. Як план лікування було встановлено в одній сесії повторне лікування через канал та хірургічне ущільнення перфорації.
Перед анестезією та ізоляцією було розпочато ендодонтичний доступ через канал, для видалення гутаперчі використовувалися фрези Gates-Glidden (Maillefer / Dentsply, Ballaigues, Швейцарія) # 2 та # 3 на низькій швидкості. Залишковий матеріал заповнення, найближчий до перфорації, був видалений за допомогою файлів типу Hedströem (Maillefer / Dentsply, Ballaigues, Швейцарія) та рясно промивався фізіологічним розчином. Потім вхід каналу був ущільнений тимчасовим заповнювальним матеріалом.
Хірургія параендодонтії розпочалася з асептики операційного поля, розрізу, підняття модифікованого клаптя Ньюмена, остеотомії та кюретажу зони перфорації. Використовувалася рясна іригація фізіологічним розчином для підготовки порожнини, після чого було проведено сушіння. Потім було здійснено ущільнення перфорації та реконструкцію вестибулярної стінки каналу з додаванням мінерального тріоксиду (MTA Productos Angelus Dental, Лондрина, Бразилія) за допомогою ручних конденсаторів та вологих ватних кульок (Рис. 6). Повернутий клапоть був зашитий плетеним шовком 3.0.
Нарешті, через канал було виконано заповнення обтуратора MTA, закривши вхід у канал іономером скла (Ketac Molar Easymix 3M ESPE).
Пацієнт прийшов на післяопераційний контроль через 7 днів для зняття шва, і було підтверджено, що протягом цього періоду він не мав симптомів. Під час клінічної оцінки через 12 місяців було виявлено клінічну тишу, відсутність больової симптоматики, фістули або вестибулярного набряку, а періодонтальні зонди були в межах нормальних значень. Рентгенографічно можна спостерігати відсутність радіолucidних зон або навколишньої втрати кістки.
Обговорення
Іміджологія є важливим інструментом для досягнення точного діагнозу на основі клінічних гіпотез. Це дозволяє фахівцеві встановити відповідний і точний план лікування. У багатьох випадках перфорації виявляються за допомогою періапікальних рентгенівських знімків, однак використання рентгенівської оцінки як єдиного засобу для виявлення та класифікації кореневих перфорацій є однією з найважливіших обмежень для клініциста. Рентгенівське виявлення зазвичай є складним і неточним, особливо коли дефект розташований на вестибулярній або язиковій стороні кореня. Щоб подолати ці обмеження, використовували комп'ютерну томографію об'ємного типу, яка забезпечує кращу візуалізацію анатомічних областей у трьох вимірах та наявності патологій, які часто не виявляються за допомогою звичайної рентгенографії. У даному випадку не було б можливим встановити діагноз вестибулярної перфорації без оцінки тривимірних зображень.
Частота, з якою відбуваються перфорації та їх місцеві пошкодження, як структур зубів, так і підтримуючих структур, викликала велике занепокоєння у дослідників, оскільки вони є важливою причиною ендодонтичних невдач. Відповідно до Fuss і Trope, ми вважаємо, що високий відсоток іатогенних кореневих перфорацій, про які повідомляється в літературі, може бути зменшений у майбутньому, оскільки ендодонтичні лікування, особливо випадки кривих і вузьких кореневих каналів або зубів, які мають незвичайні системи кореневих каналів, будуть виконуватися професіоналами з достатньою попередньою підготовкою.
Прогноз для перфорованого зуба залежить від: місця перфорації, часу, протягом якого вона дозволяє забруднення, можливості її герметизації та доступності основного каналу.
Беручи до уваги клінічний та рентгенологічний аспекти, представлений випадок має особливість швидкого вирішення після трьох тижнів травми, з точним діагнозом та технікою, яка включає герметизацію перфорації та одночасне встановлення бар'єру з MTA на одній зустрічі.
Д. Едгар Вальдівія, Маріо Ф. де Паскуалі Леонардо, Мануел Е. де Ліма Мачадо
Бібліографія
- Пател С, Дауд А, Пітт Форд Т, Уайтес Е. Потенційні застосування конусної комп'ютерної томографії в управлінні ендодонтичними проблемами. Int Endod J. 2007;40:818-3.
- Естрела К, Буено МР, Лелес КР, Азеведо Б, Азеведо JR. Точність конусної комп'ютерної томографії та панорамної і періапікальної рентгенографії для виявлення апікального періодонтиту. J Endod. 2008;34(3):273-9.
- Пател С. Нові виміри в ендодонтичній візуалізації: частина 2. Конусна комп'ютерна томографія. Int Endod J. 2009; 42(6):463-75.
- Коттон ТП, Гейслер ТМ, Холдена ДТ, Шварц СА, Шиндлер ВГ. Ендодонтичні застосування конусної об'ємної томографії. J Endod.2007;33(9):1121-32.
- Селтцер С, Бендер ІБ, Сміт Дж, Фрідман І, Назімов Г. Ендодонтичні невдачі: аналіз на основі клінічних, рентгенографічних та гістологічних даних-I. Oral Surg Oral Med Oral Pathol. 1967;23:500-16.
- Вайгер Р, Аксманн–Крчмар Д, Лост С. Прогнозування традиційного лікування кореневих каналів переглянуто. Endod Dent Traumatol. 1998;14:1-9.
- Інгл Дж, Бакленд Л. Ендодонтія; Ендодонтичні ускладнення: їх виявлення, корекція та профілактика. 5-е видання, Видавництво: McGraw-Hill Interamericana. Мехіко, Д.Ф. 2004: 856-868.
- Синай ІГ. Ендодонтичні перфорації: їх прогноз і лікування. J Am Dent Assoc 1977;95: 90–95.
- Селтцер С, Синай І, Август Д. Пародонтальні ефекти перфорацій коренів до і під час ендодонтичних процедур. J Dent Res 1970;49:332-9.
- Гарріс ВЕ. Спрощений метод лікування ендодонтичних перфорацій. J Endod 1976;2:126-34.
- Фус З, Тропе М. Перфорації коренів: класифікація та вибір лікування на основі прогностичних факторів. Endod Dent Traumatol 1996;12:255- 64.
- Біггс ДжТ, Бененаті ФВ, Сабала КЛ. Лікування іатроґенних перфорацій кореня з супутніми кістковими ураженнями. J Endod 1988;14(12): 620-4.
- Цесіс І, Фус З. Діагностика та лікування випадкових перфорацій кореня. Endod Topics. 2006;13(1):95-107.
- Лемон, Р.Р. Нескальпельний ремонт дефектів перфорації: концепція внутрішньої матриці. Dent. Clin. North Am., 1992;36,439-457.
- Рода РС. Ремонт перфорації кореня: хірургічне та нехірургічне управління. Pract Proced Aesthet Dent 2001;13(6):467–72.
- Кастеллучі А. Збільшення в ендодонтії: використання операційного мікроскопа. Pract Proced Aesthet Dent 2003;15:3