
en
An etiological approach to mesial relationships
9
14 хв читання
05 червня 2025
Машинний переклад
Оригінальна стаття написана мовою ES (посилання для прочитання).
Mesiorrelations are the syndrome that presents in the consultation with less frequency. However, when the child presents with a concave profile, with sunken cheeks, with superior retrognathia, inferior prognathism and/or progeny, we are filled with concern. We are filled with concern because we know that an easy task awaits us, because we have been taught that we may encounter a "true" class III, one of those that resist all therapeutic attempts, and end up in orthognathic surgery.
However, our teachers and our experience have taught us that not all mesiorrelations are the same; that the old classification of "true" and "false" is highly incomplete and, more importantly: "any mesiorrelation treated at the right time; during growth ages, can be resolved."
We said that in growth ages there are always possibilities for a solution, but only if we are able to find in each case what is the cause that produced the syndrome. That is to say, we have a syndrome: the mesiorrelation, with all its signs and symptoms; to make an etiological diagnosis we must find the cause, and thus have an etiopathogenic view of the problem.
This analysis of the mesial relationship is the only one that will allow us to hit the precise key and walk the correct path to reverse the process.
What are the main parameters we should analyze?
- The sizes of the maxillae (upper and lower).
- The anteroposterior position of the maxillae in relation to the base of the skull and to each other.
- The dental axes.
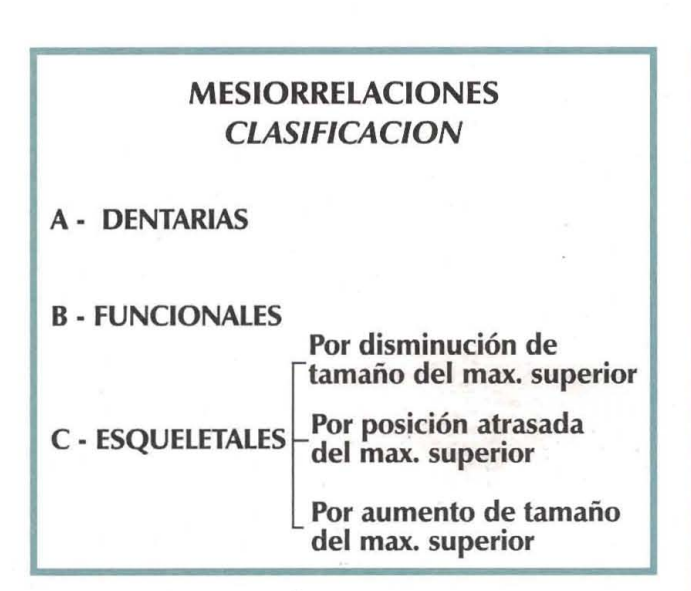
So, in the face of a mesiorrelation, the challenge is to find out what the main altered factor is, what alteration allowed the entire syndrome to establish itself. We understand that five well-defined situations can occur:
- Cases in which the main alteration is in the abnormal inclination of the axes of the incisors, while the rest of the parameters remain more or less close to normal. This is referred to as a DENTAL MESIORRELATION or an ANterior CROSSBITE.
- Cases in which there is a mandibular advancement due to premature contact in the anterior sector, with the other parameters being normal. We then define it as a FUNCTIONAL MESIORRELATION or PROSLIDING. The diagnosis in this case must be primarily made clinically, looking for the contact point.
- When deep structures are compromised, we are faced with SKELETAL ALTERATIONS.
We can find:
- Reduced size upper jaws.
- Upper jaws located in a backward position relative to the base of the skull.
- Enlarged mandibles.
In general, we find more than one altered element in each case, so we must take the parameter that deviates the most from the "should be" and direct our therapy towards that.
It is in vain to say that the vast majority of the time these children present functional disorders. Among the most common are mouth breathing and low tongue posture, dysfunctions that "per se" increase the growth patterns in the lower jaw and deprive the middle third of the face of these same patterns in all three spatial dimensions. A main part of our therapeutic approach, therefore, involves functional rehabilitation, which becomes a key element when we refer to the stability of the achievements reached with the treatment.
We will now present some examples following the classification scheme previously proposed.
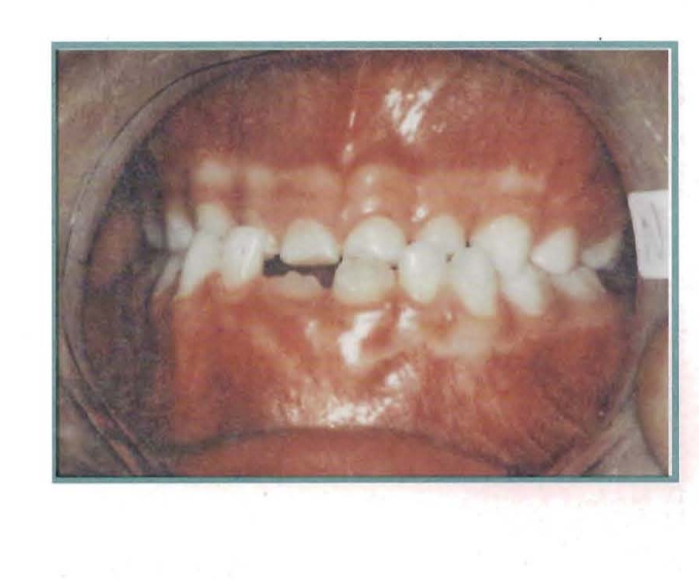
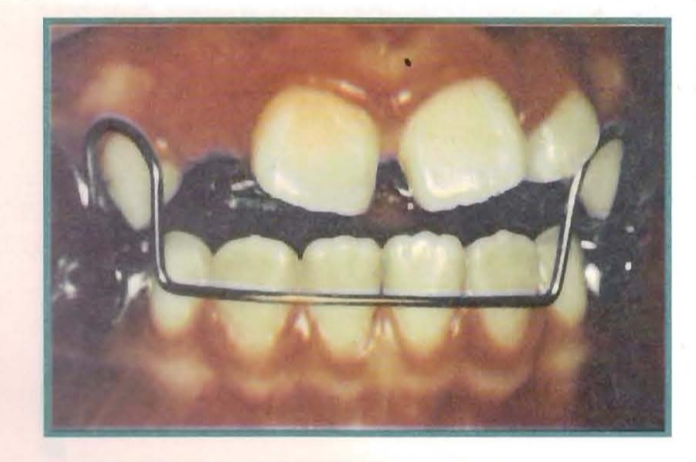
Case No. 1
Anterior crossbite or dental mesial relationship.
Patient: Juan Blas
Gender: Male
Age: 9 years
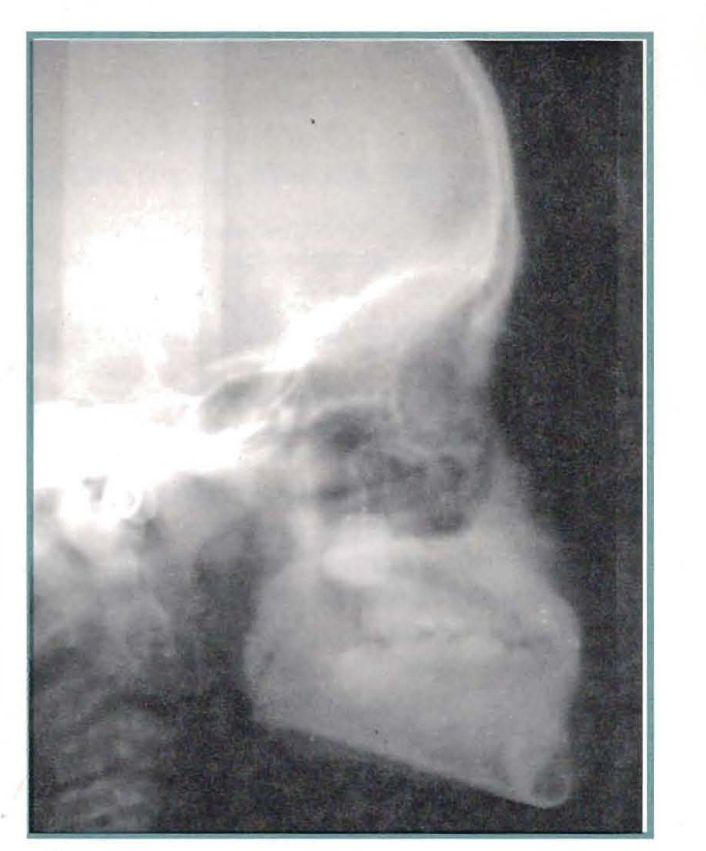
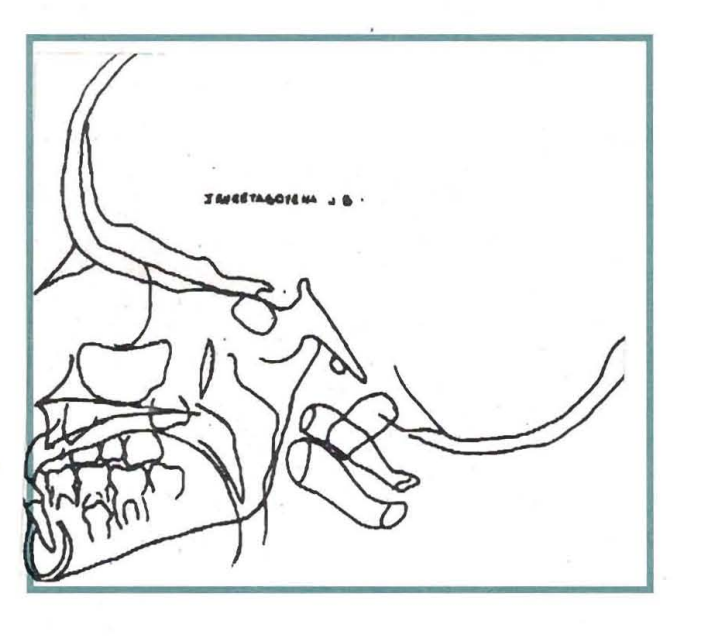
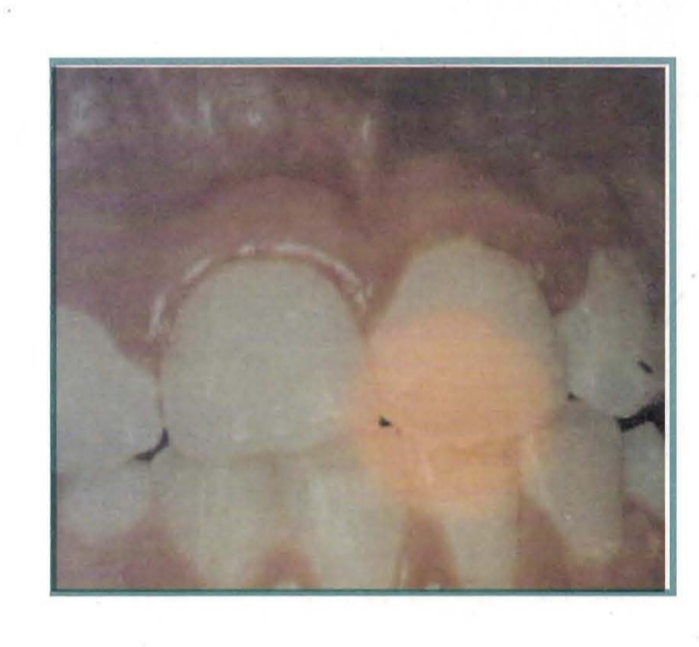
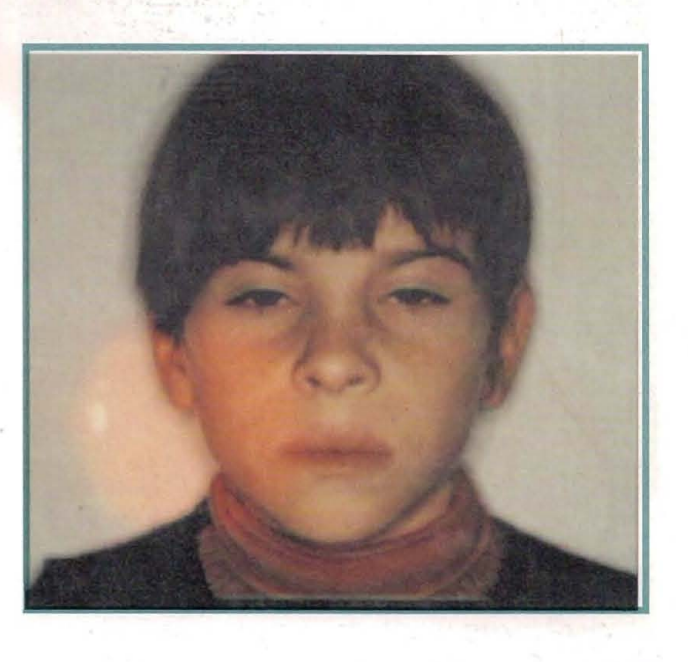
The consultation presents all the facial and dental signs of a mesial relationship.
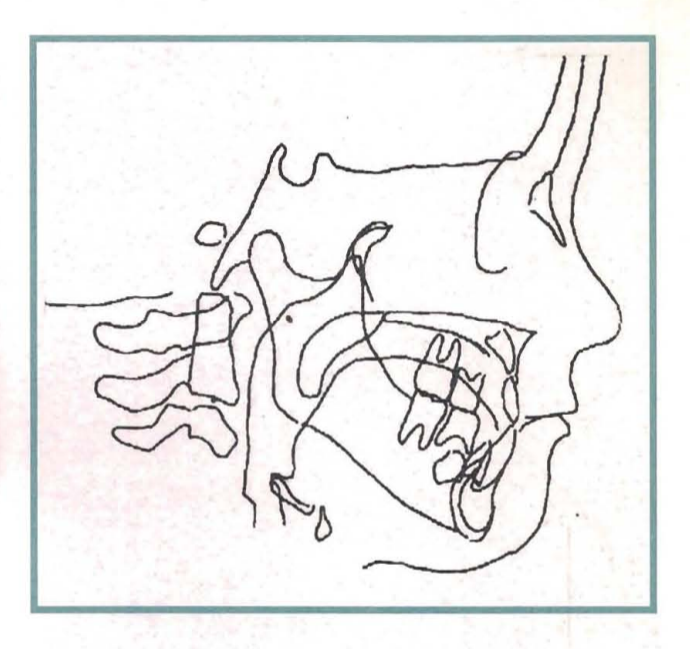
The cephalometric study reveals that the upper jaw is 1 mm less than "it should be," a finding that is not significant, and that the mandibular size is as expected. In turn, point A forms a normal angle with the base of the skull, meaning that the spatial location of the upper jaw is normal, and the mandible in relation to the upper jaw shows a slight advancement.
The most altered parameter is the axis of the lower incisor concerning the mandibular plane, showing a noticeable protrusion, which ultimately determines and defines the installation of the syndrome.
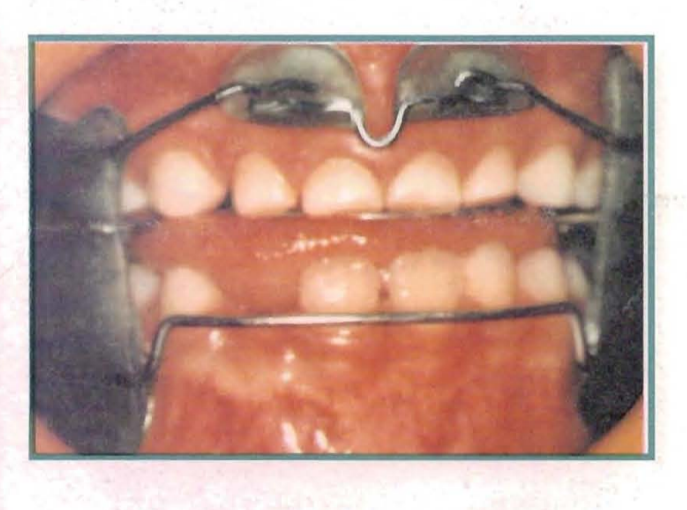
Consequently, a therapeutic element capable of normalizing the axes is used, in this case, an inclined acrylic plane that resolved the situation in just three weeks.





Case No. 2
Functional mesiorrelation or proslip
Patient: Facundo Alvarez
Gender: Male
Age: 9 years
The patient presents to the consultation with mild facial signs suggesting a mesiorrelation syndrome.
In contrast, the dental signs are evident: anterior crossbite, and class III canine and molar relationships.
When performing the clinical analysis, a premature contact is detected in the anterior area that defines the functional mesial relationship or pro-sliding.
The cephalometric analysis shows us a J angle of 79º and an F angle of 80º, which indicates a normal maxilla in its anteroposterior position with respect to the base of the skull.
Likewise, the size of the maxilla is normal (it should be 48.6 mm and is 48 mm). We are concerned about the mandibular size, which is 3 mm larger than expected. We believe that being deprived of the physiological containment of the maxilla, it has grown excessively, influenced by the low posture of the tongue.
Finally, the dental axes show us an upper incisor with an angulation of 65º, which retains the characteristics typical of eruption, and an angle for the lower incisors of 95º, which have been compromised by the inclined plane offered by the premature contact.
In light of the described analysis, it is decided to act through a dynamic functional appliance, such as the Bimmler C.
Having made an accurate diagnosis, and consequently used an appropriate therapeutic means, given the level of involvement that the lesion presents, the case is resolved in just 30 days.







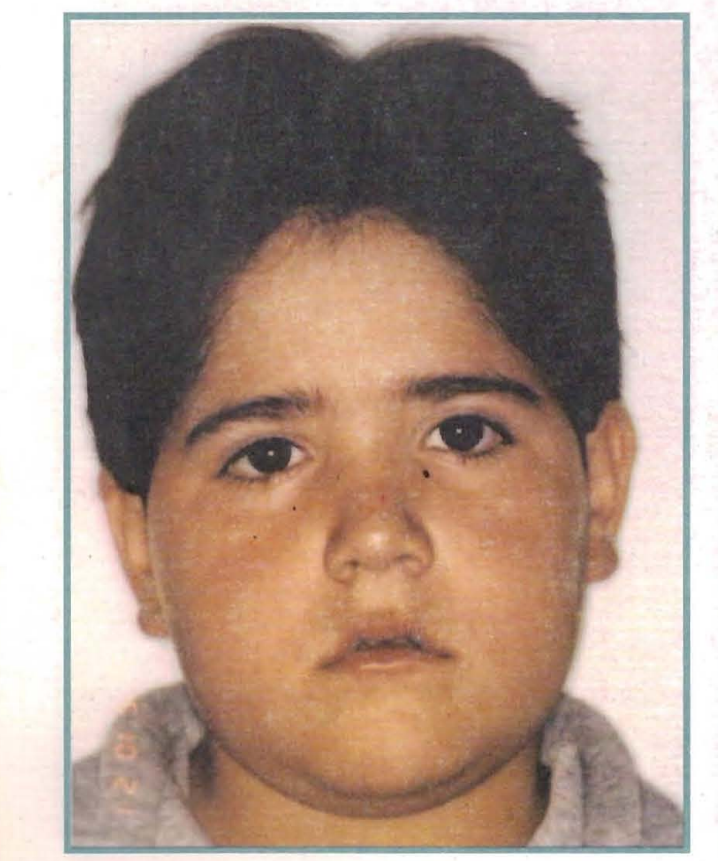
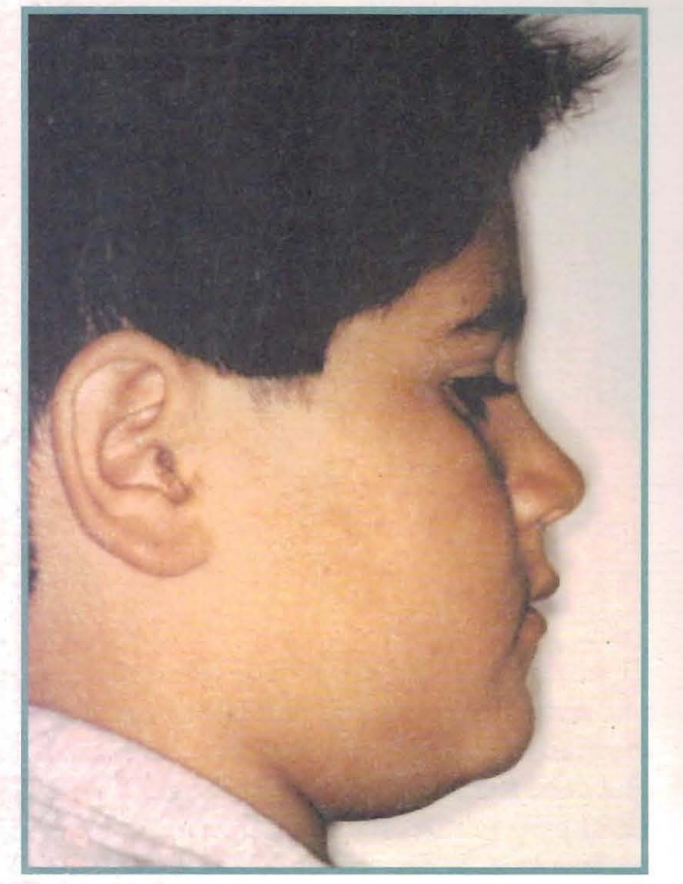
Case No. 3
Mesiorrelation at the expense of a decrease in upper jaw size
Patient: Pablo Lezcano
Gender: Male
Age: 6 years and 1 month
Pablo Lezcano was received in
Neuquén in 1993, with a mesiorrelation syndrome much more severe than his features suggested.
The clinical study showed that we needed to look for alterations in deeper planes than a simple inclination of dental axes.
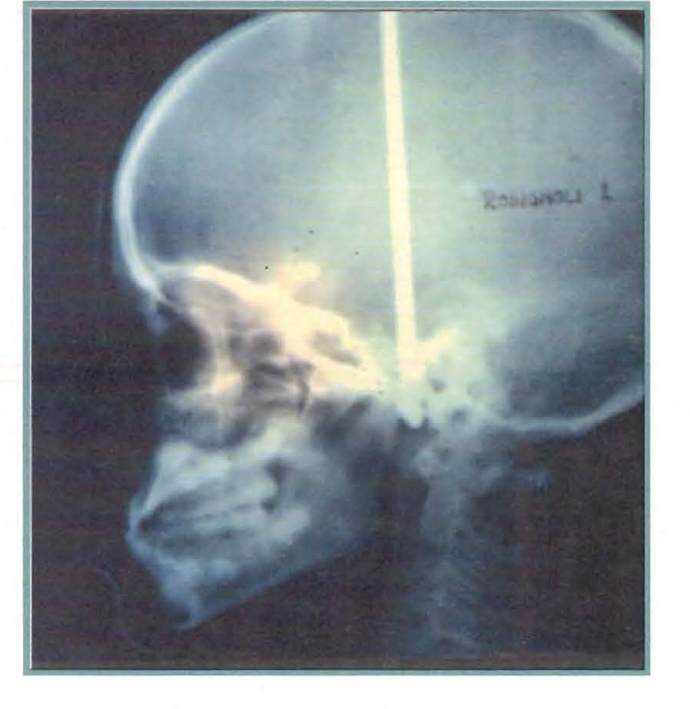
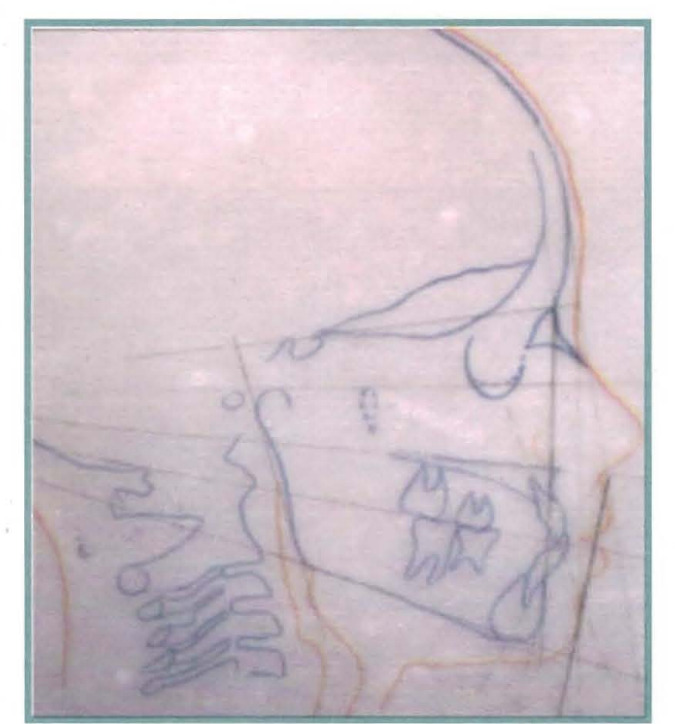
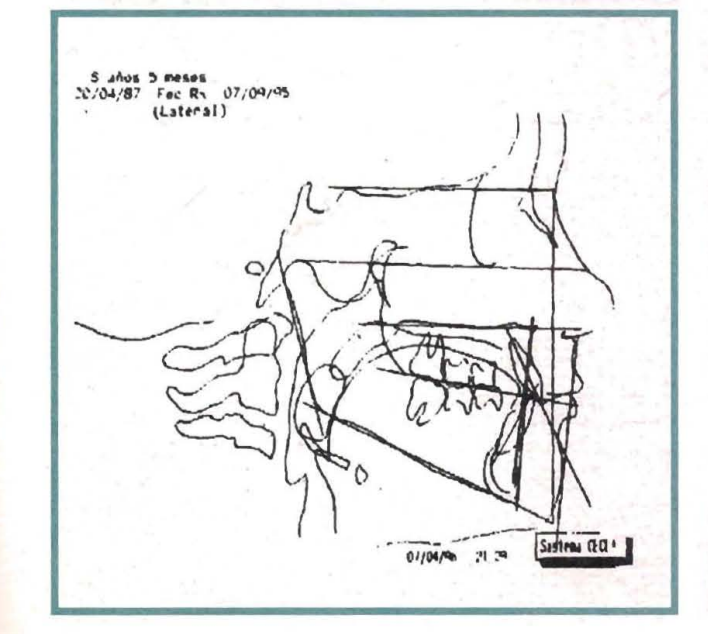
Thus, the cephalometric analysis indicates a decrease in the size of the upper jaw by 6.6 mm compared to what it should be. Although there is also a deficit in the position of the upper jaw concerning the base of the skull, it is very small, enough not to prompt us to act on that factor. The other factors are normal.
Once this analysis was done, we thought that the Function Regulator III was the indicated therapeutic element, focusing on the rearrangement of the periosteal matrices, particularly in this case the traction of the Lathan Ligament.
We worked with the RRIII for several months, observing the change in position of the germs of the upper incisors.
Finally, after 28 months of treatment, we achieved the alignment of the anterior sector and the maxillomandibular anteroposterior relationships.
We want to point out that two years and three months later, we have achieved an increase in the length of the upper jaw by 5.6 mm, while the rest of the parameters remain within the norm.
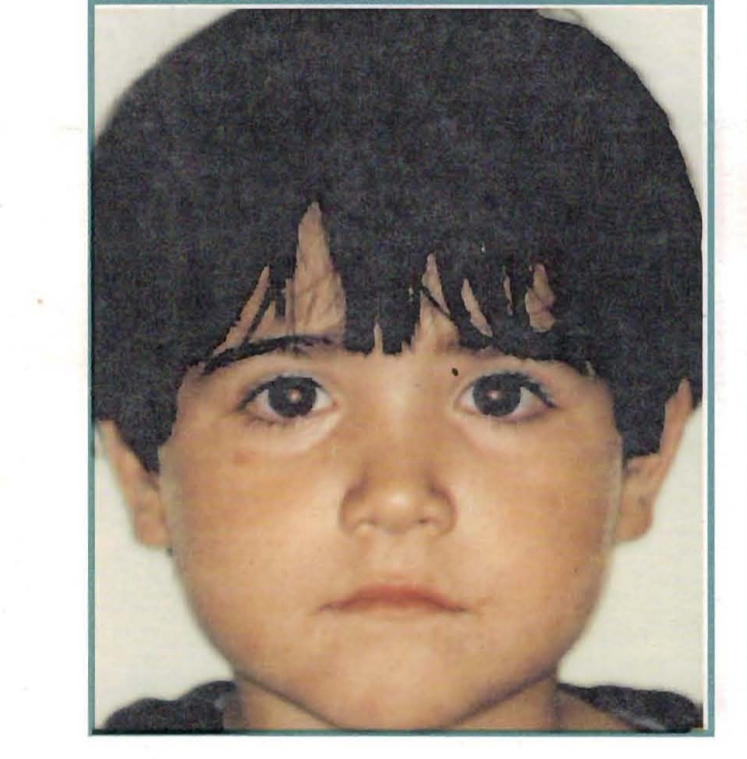
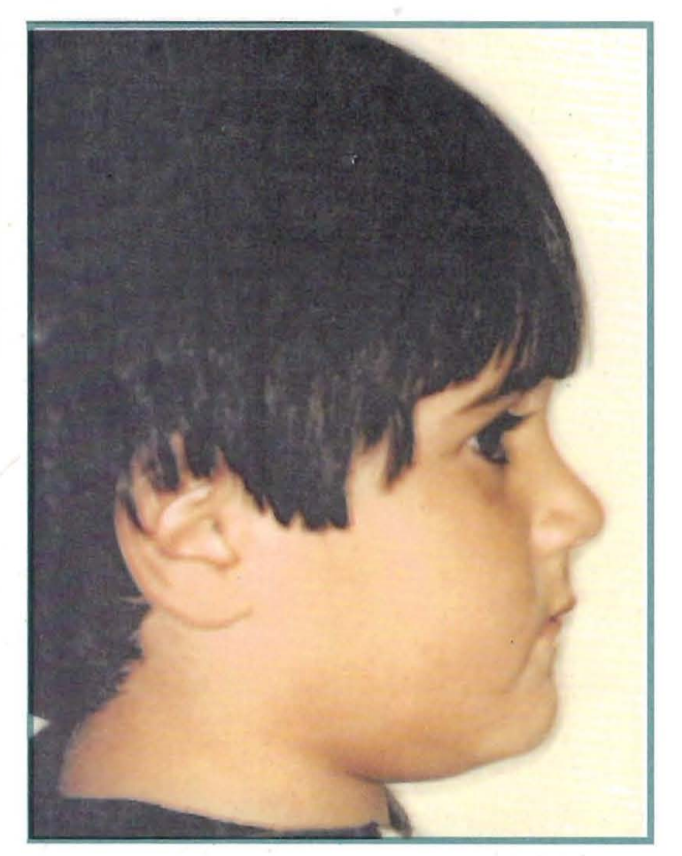






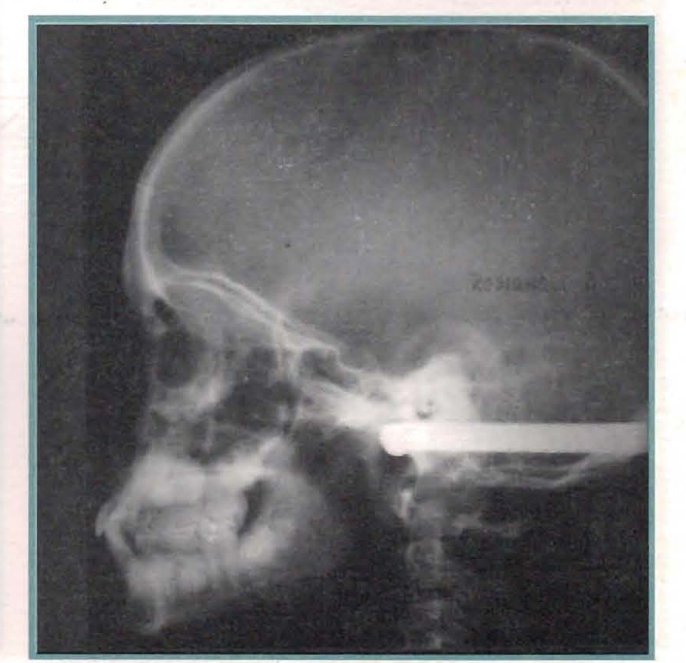
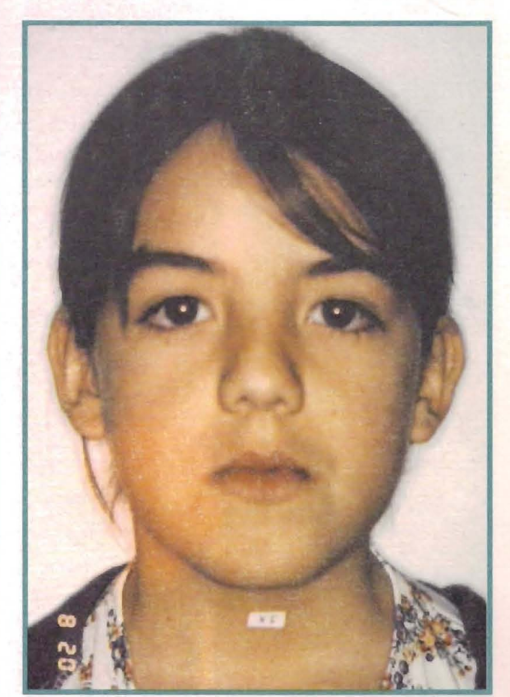
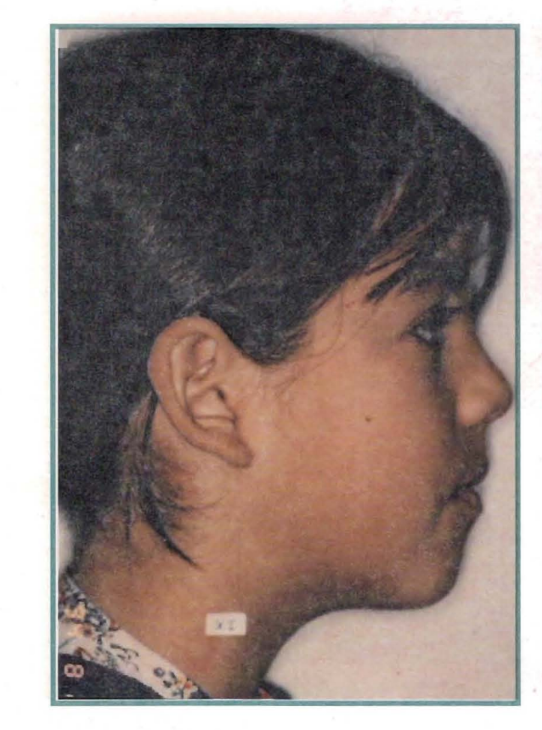
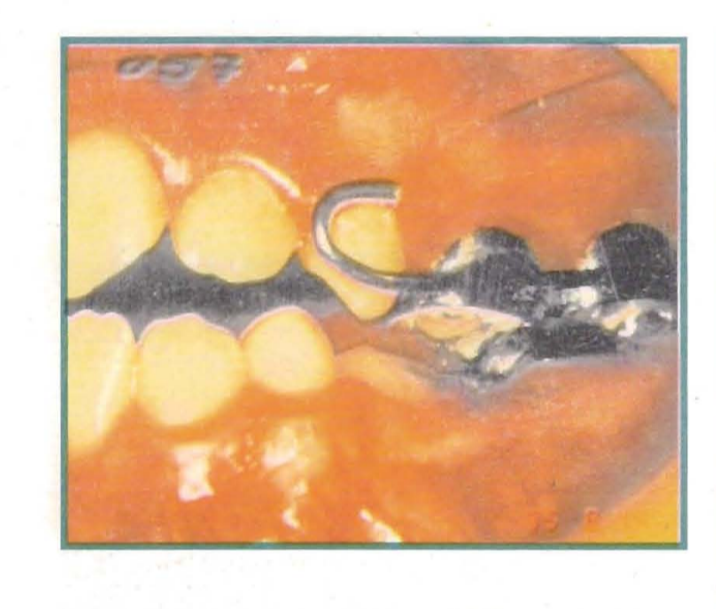
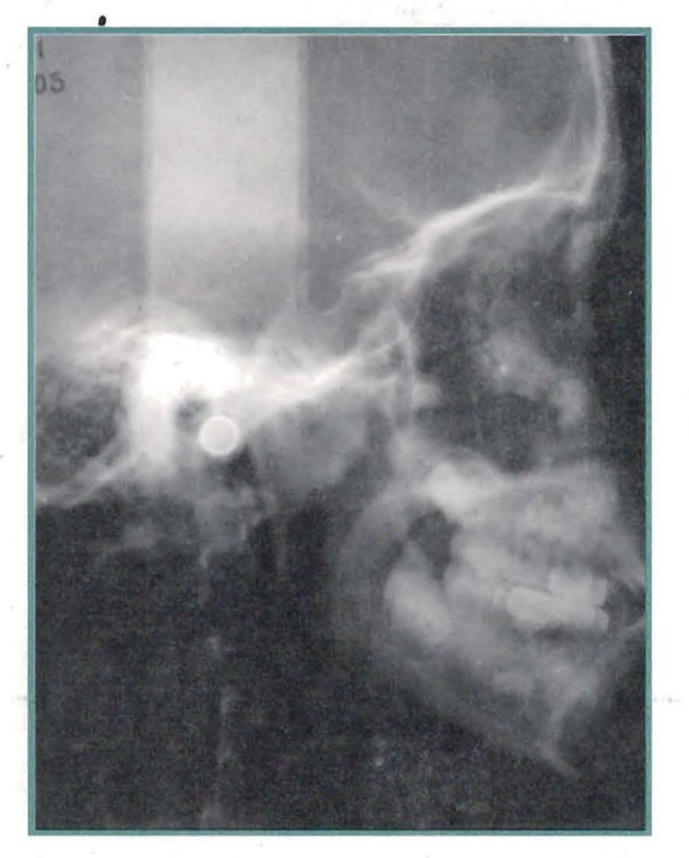
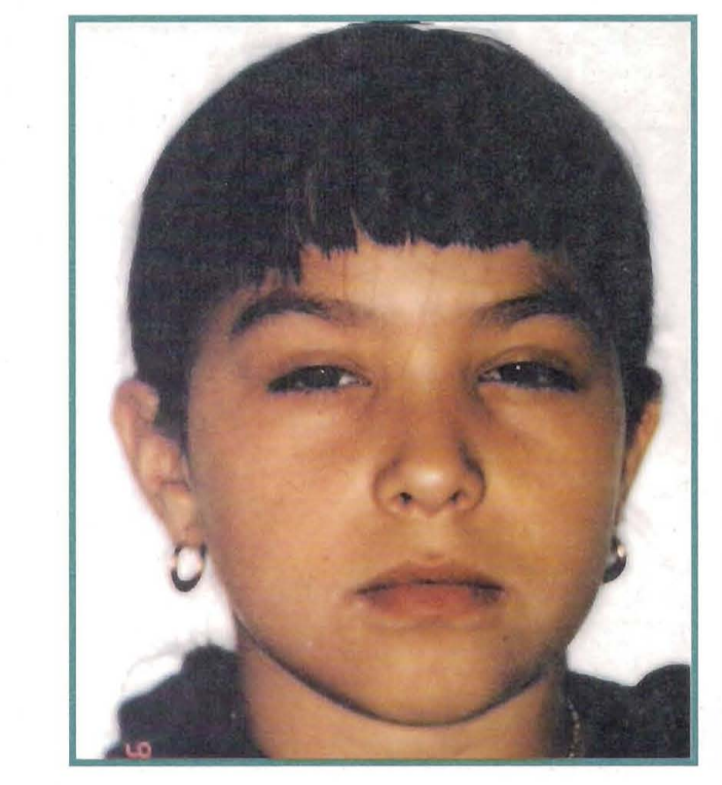
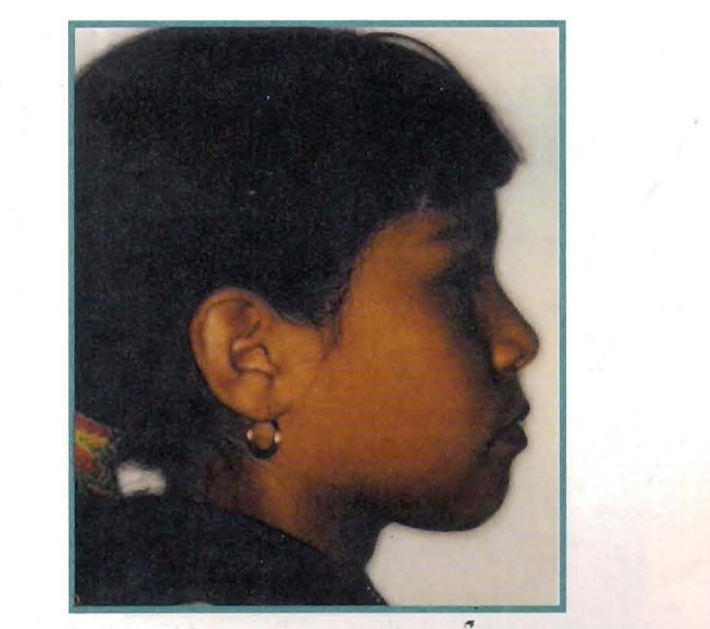
Case No. 4:
Delayed position of the maxilla with respect to the cranial base.
Patient: Cintya Escalona
Gender: Female
Age: 9 years
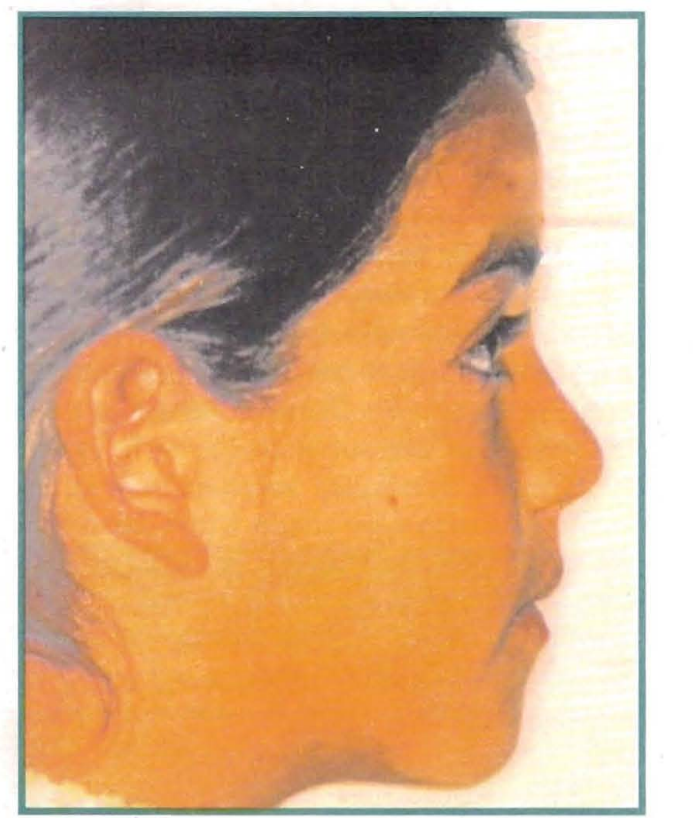
Cintya arrives at the course from a colleague's private practice, who is concerned about the severity of the case.
The facial analysis presents the classic signs of mesio-relations.
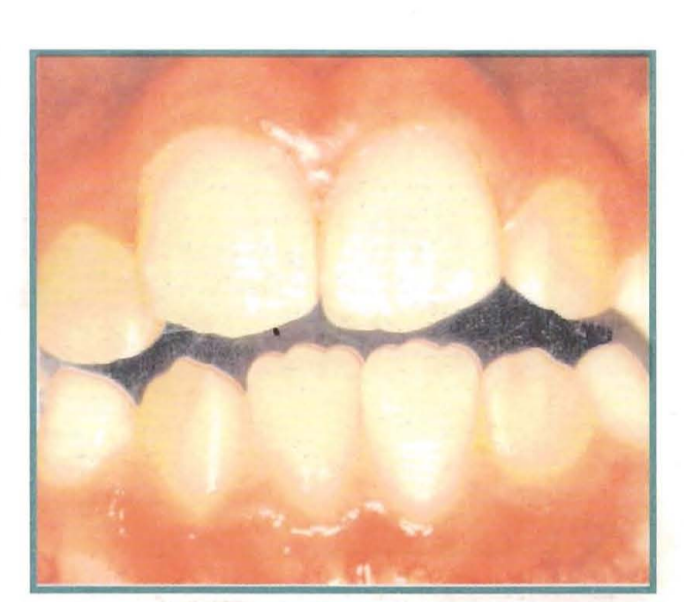
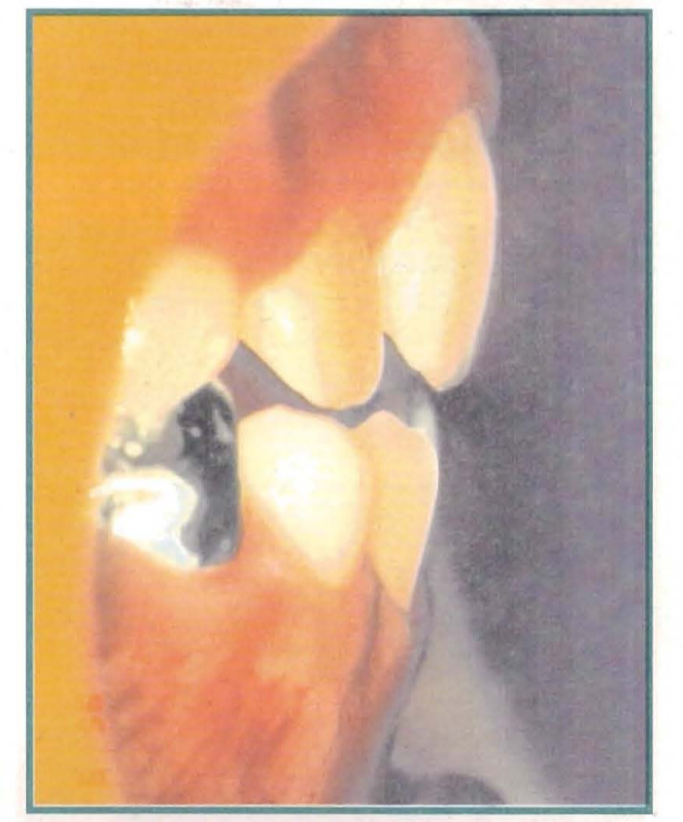
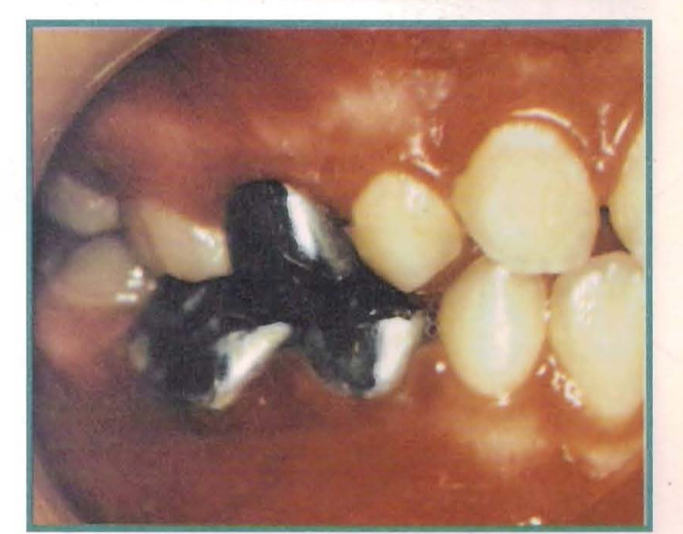
On clinical inspection, there is a true collapse, both transverse and anteroposterior of the maxilla, with an anterior step of 4 mm, and bilateral posterior crossbite.
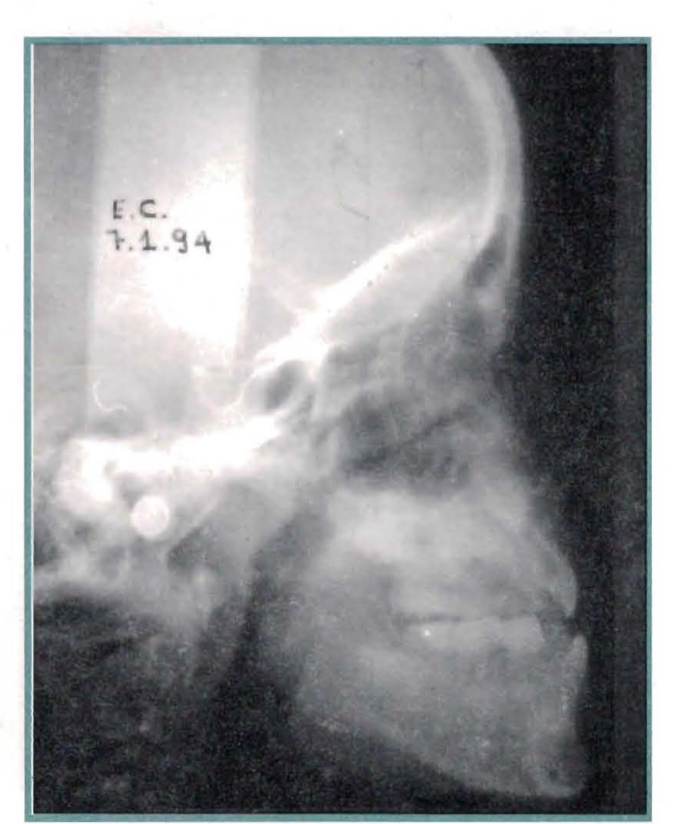
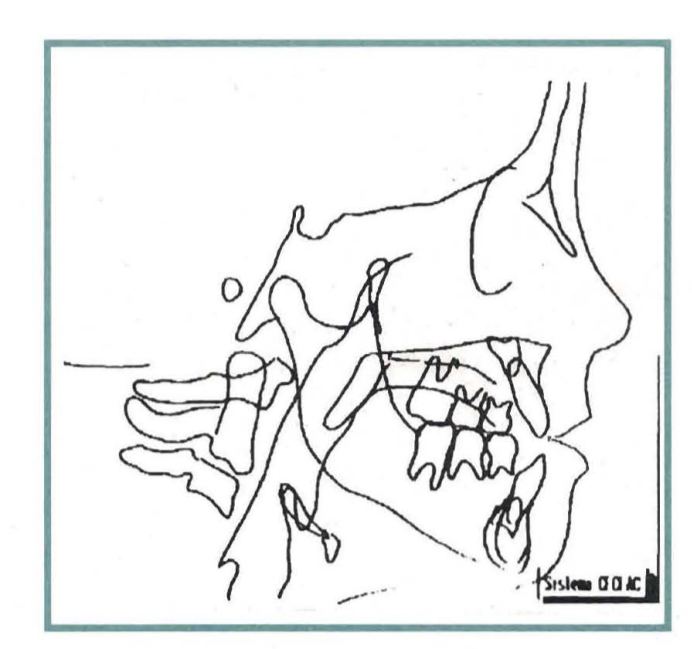
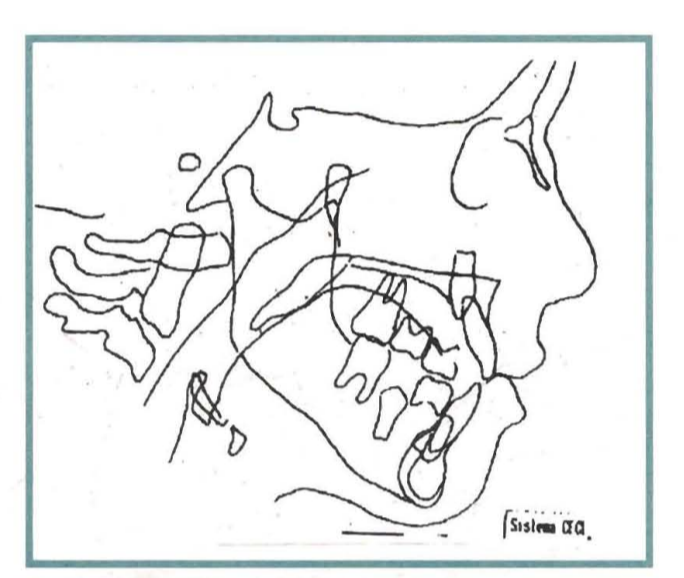
The cephalometric study shows a deficit of 5° in the position of the maxilla with respect to the cranial base, although we also observe a decrease of 3.5 mm in size. Of course, the position of the mandible is advanced, but fortunately its size is smaller than expected.
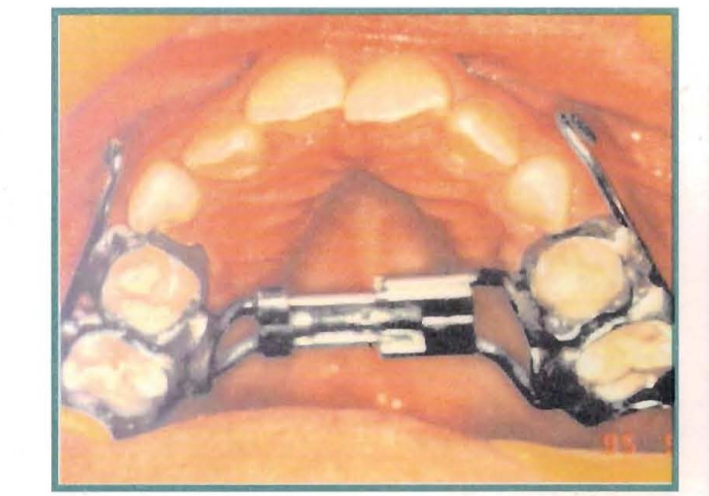
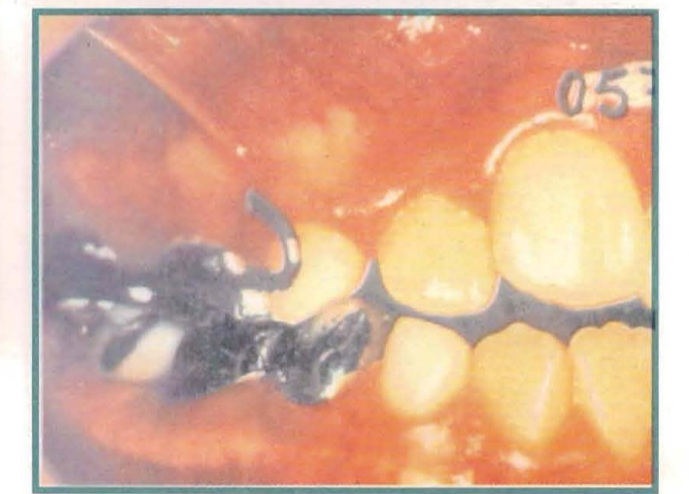
The magnitude of the deficits in the transverse diameters, and the characteristic of the dental axes, parallel to the bony bases, led us to appeal to the responsiveness of the midpalatal suture, and we then performed a transverse disjunction. The posteriorly positioned maxilla required anteroposterior traction with a Delaire mask. Thus, a disjunctor is constructed, to which a sectioned vestibular gutter is added, with the classic grips for elastics at the mesial level of the canines. Work is done in both transverse and anteroposterior directions at the same time, resolving the normalization of the transverse diameters in just under a month.
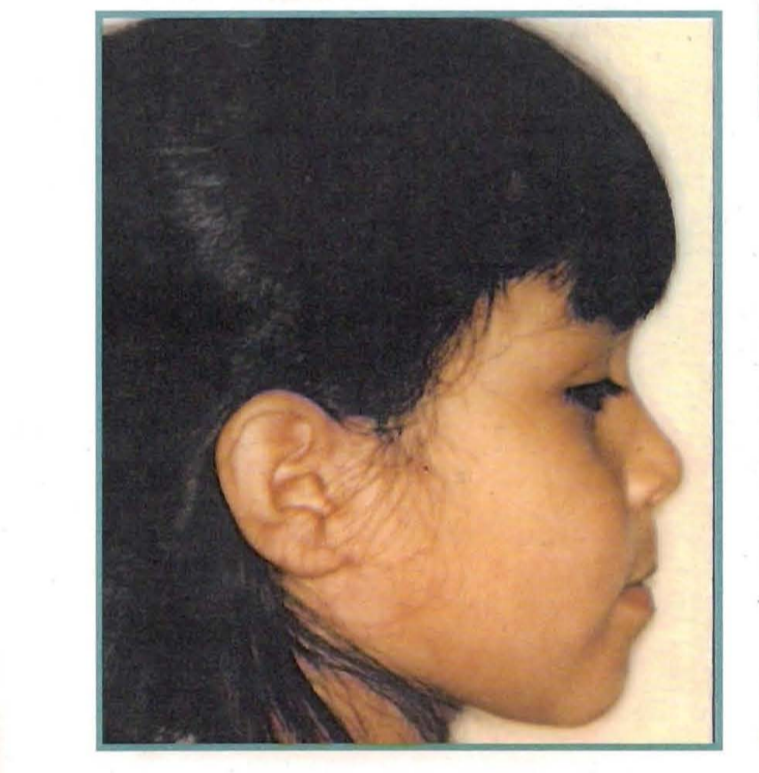
One and a half years later, the antero-posterior aspect is resolved, although there is still a vertical deficit.
The cephalometric analysis at that moment shows us that there is still a slight delay of the upper jaw with respect to the base of the skull, that the length of the mandible is below the expected limits, and that we can still appeal to the growth of the premaxilla to fully compensate for the antero-posterior relationships.


Case No. 5:
Mandibular size increase
Patient: Johatia Tapia
Gender: Female
Age: 4 years 9 months
The patient presents to the consultation referred by the Pediatric Dentist, who, upon seeing the severity of the case, demands the consultation and eventually the treatment, despite the young age of the girl. The clinical analysis told us little about the etiology of the case, although there are two points to mention: the soft subnasal point does not appear sunken in profile and a double chin is observed, resulting from a low tongue posture.
When observing the arches, we see an anterior reverse bite and sagittal relationships of mesial relationship, with class III also observed in the canine and molar key.
It is by conducting the cephalometric study that we find the alterations that configured this syndrome. As observed, the position of the maxilla in relation to the base of the skull is practically normal, and the size of the maxilla exceeds what is expected. It is the size of the mandible, with 4 mm of excess over what is expected, where we find the answer we are looking for.
We then find ourselves facing a mesial relationship due to an increase in the size of the mandible.
Fortunately, the patient is just under five years old, and we focus on resolving the case by appealing to the remodeling of the alveolars. A Blimmer C is installed.
After a year, another cephalometric evaluation is conducted, where it is observed that the mandible has continued to grow, perhaps following genetic patterns.
Notwithstanding the above, the clinic shows a harmonious morphofunctional balance.
The objective of this communication has primarily been to highlight that whenever we can reach the cause of our misrelationship, it is possible to resolve it at appropriate ages.





Summary
The mesiorrelations are classified into three types:
- Dental
- Functional
- Skeletal
- by reduction in the size of the maxilla.
- by the posterior position of the maxilla.
- by an increase in the size of the mandible.
Each of them is exemplified with a clinical case, showing that in growth ages and targeting the therapy to resolve the most altered factor, it is possible to correct the different clinical varieties of this syndrome.
Graciela I. Lorenz, Norma Rivas, Aniérico Ceccarelli
Bibliography:
- Timely diagnosis and therapeutic management of mesiorrelations. Dr. B.G. de Segré. Rey. of the AAO.F.M. Vol. 17 No 53-54. July 1984-June 1985.
- The Delaire mask in the treatment of Class III. Drs. A Maxciandaroy B.de Bellis. Rev. Advances in Odontoestomatology 1992-8:279-286.
- Postero-anterior traction in Class III malocclusions. Dr. J. Cortes B. Rev. A O.A. July 1979.
- Delaire J. et al: "Some results of extraoral distractions supported by the mentonier in the orthopedic treatment of maxillomandibular malformations of Class III and the sequelae of labiomaxillary clefts. Revue de Stomatologie (Paris) 73:633-642-1972.
- Verdon P "New orientations in orthodontic treatments of maxillodental sequelae of total labio-maxillary clefts with palatine division. Ortod. Fr. 45: 11-66 1974.
- Delaire, J. Construction of the orthopedic mask. Revue de Stomatologie. 72:579-582. 1971.
- Delaire J. "The growth of the face. Rev. Fr. Odontoestomatologie XIX-364-391 -1972.
- Petrovic, A: "Biological analysis of the control processes of postnatal growth of the mandible and maxilla. Ed. Julien Prelat. Paris 1975.
- Delaire J.: The mandibular prognathism syndrome. Orthod. Fran. 47:203-1976.
- Frankel, R: "Maxillary retrusion in Class III and treatment with the functional corrector III. Eur. Orthod. Soc. Trans. 1970.
- Graber TM., Petrovic A; Dentofacial Orthopedics with functional appliances. G. V Mosby, St. Louis. 1985.
- Blitner Von. H. Trans. Pedro Loverstein. New viewpoints on the etiology of progeny. Rey. MOFM. July '80-June '81. 14:71-80.
- Graber-Swain. Orthodontics. 1968.
- Torres Ramón. Ifratado de Gnato-Ortopedia funcional. 1966.
- Guardo A, Guardo G.R. Orthodontics. 1981.
- Graber-Newman. Orthodontic Appliances. 1987.